
Surface and Radiological Anatomy — MCQs

On this page
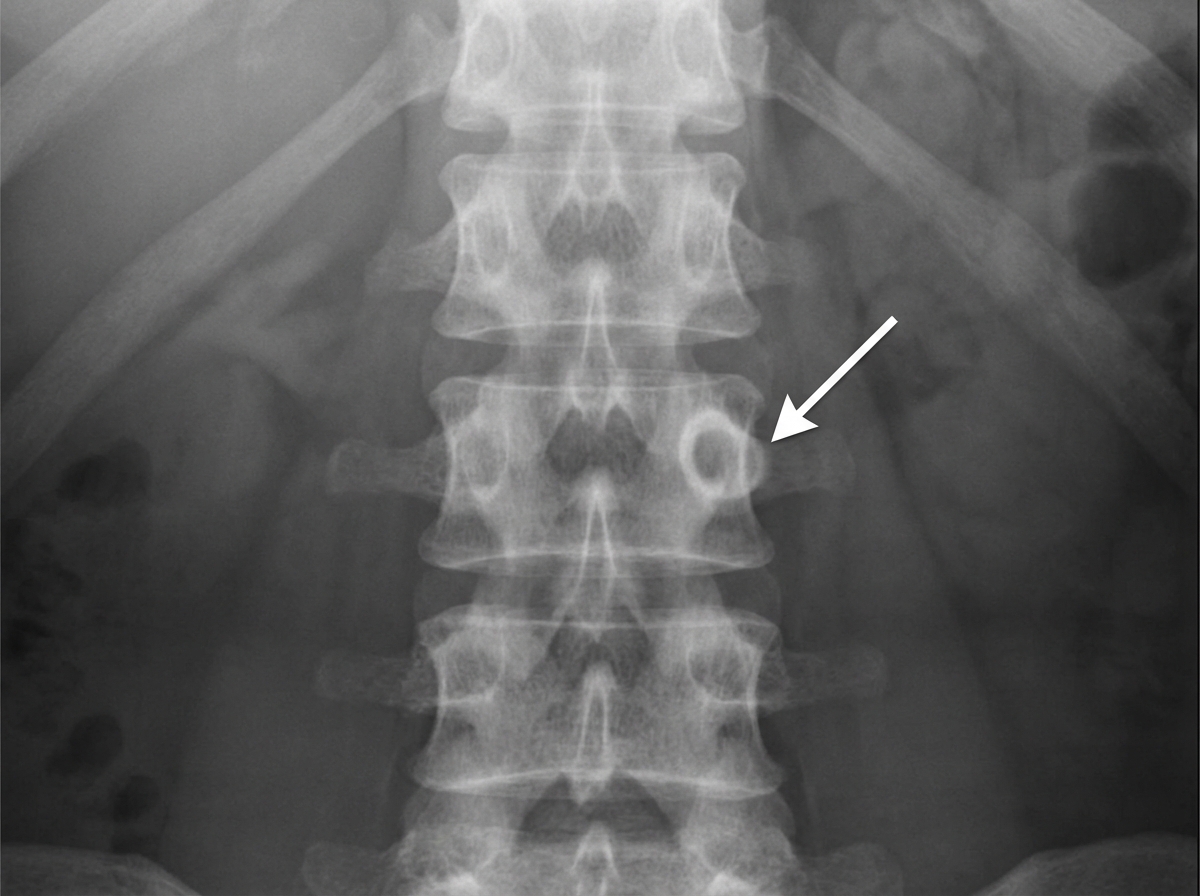
Which anatomical structure is characterized by a worm-hole radiolucency?
In the provided X-ray, what anatomical structure is indicated by the marked region?
Sappey's line denotes a line encircling which anatomical region?
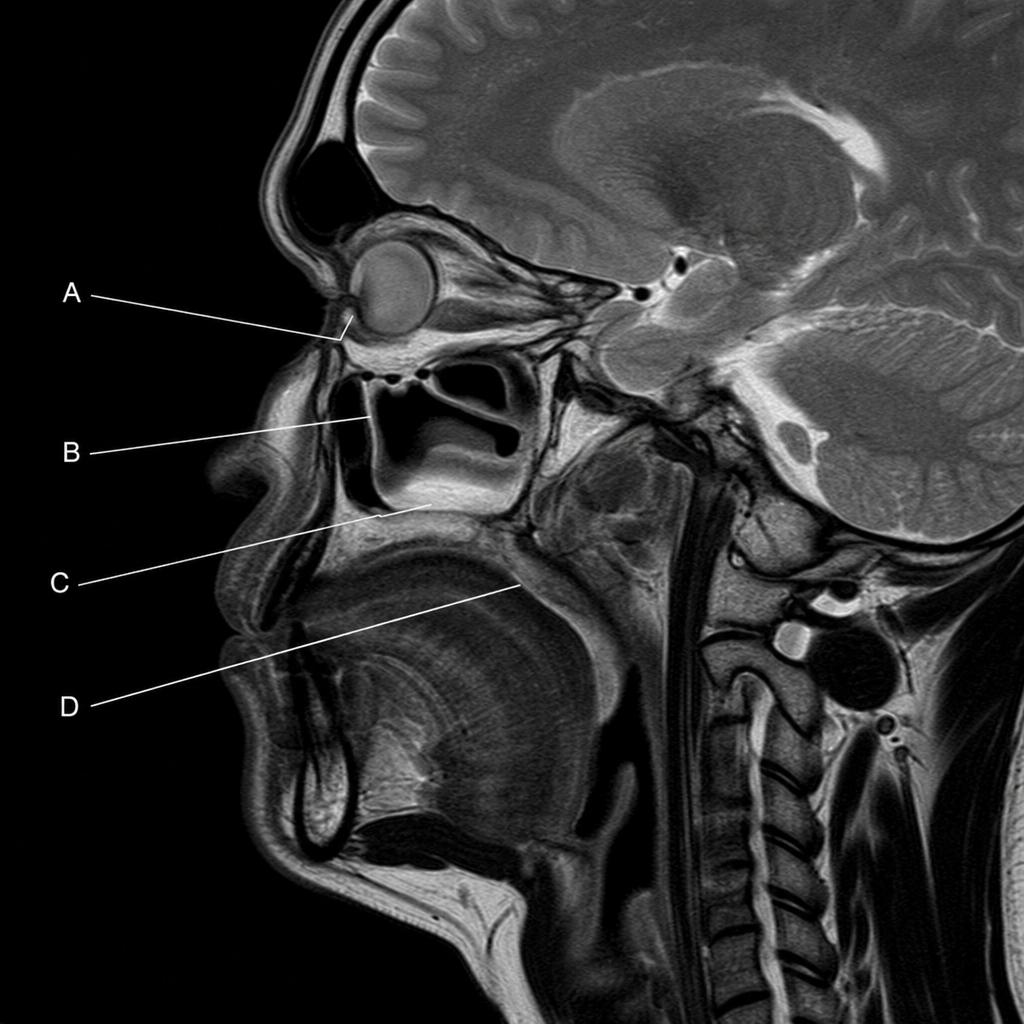
In an MRI scan showing a sagittal section through the head and neck, tears drain through the nasolacrimal duct into the space below which structure?
Which sinus is the last to appear radiologically on X-ray?
Practice by Chapter
Surface Landmarks of the Head and Neck
Practice Questions
Surface Landmarks of the Thorax
Practice Questions
Surface Landmarks of the Abdomen
Practice Questions
Surface Landmarks of the Limbs
Practice Questions
Radiographic Anatomy
Practice Questions
CT Anatomy
Practice Questions
MRI Anatomy
Practice Questions
Ultrasonographic Anatomy
Practice Questions
Angiographic Anatomy
Practice Questions
Sectional and Cross-sectional Anatomy
Practice Questions
Anatomical Correlations in Common Imaging
Practice Questions
Interventional Radiological Anatomy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app