
Pelvis and Perineum — MCQs

On this page
Which one of the following is NOT a support of uterus, preventing its descent?
What is the volume of the prostate in normal adult males?
What can cause the absence of fructose in seminal fluid?
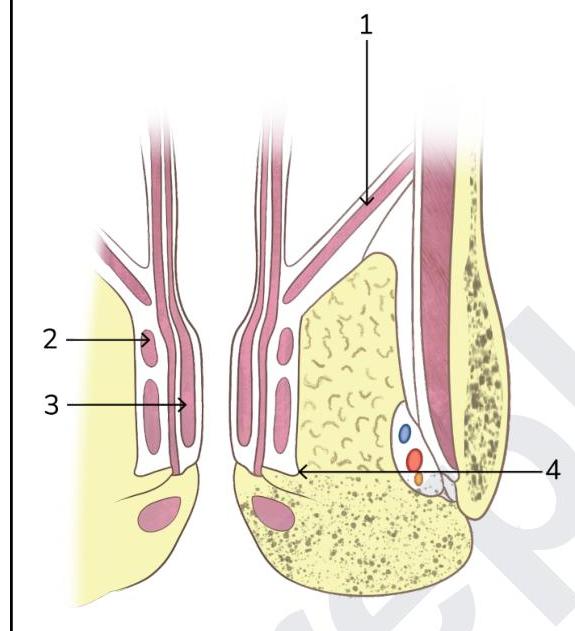
The horizontal arrow labeled 1 on the right side of the diagram points to which muscle, the principal muscular component of the pelvic diaphragm?
A 33-year-old woman comes to the emergency department because of a 1-hour history of severe pelvic pain and nausea. She was diagnosed with a follicular cyst in the left ovary 3 months ago. The cyst was found incidentally during a fertility evaluation. A pelvic ultrasound with Doppler flow shows an enlarged, edematous left ovary with no blood flow. Laparoscopic evaluation shows necrosis of the left ovary, and a left oophorectomy is performed. During the procedure, blunt dissection of the left infundibulopelvic ligament is performed. Which of the following structures is most at risk of injury during this step of the surgery?
A 13-year-old boy is brought to the emergency department by his parents for evaluation of severe groin pain for the past 4 hours. His symptoms began while he was participating in a basketball game. On arrival to the ED, the resident on call notes a swollen, tender, and elevated left testicle with absence of the cremasteric reflex. A urology consult is requested and the patient is scheduled for surgery. An abnormality in which of the following anatomical structures is most likely responsible for this patient’s condition?
Injury to which of the following muscles that forms the deep support of the perineal body causes cystocele, enterocele and urethral descent?
The length of the female urethra is :
Vaginal sphincter is formed by all except
Which of the following is present in males but not in females?
Practice by Chapter
Pelvic Walls and Floor
Practice Questions
Pelvic Viscera
Practice Questions
Urogenital Organs
Practice Questions
Pelvic Vasculature
Practice Questions
Pelvic Innervation
Practice Questions
Male Perineum
Practice Questions
Female Perineum
Practice Questions
Pelvic Lymphatics
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Gender Differences in Pelvic Anatomy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app