
Pelvis and Perineum — MCQs

On this page
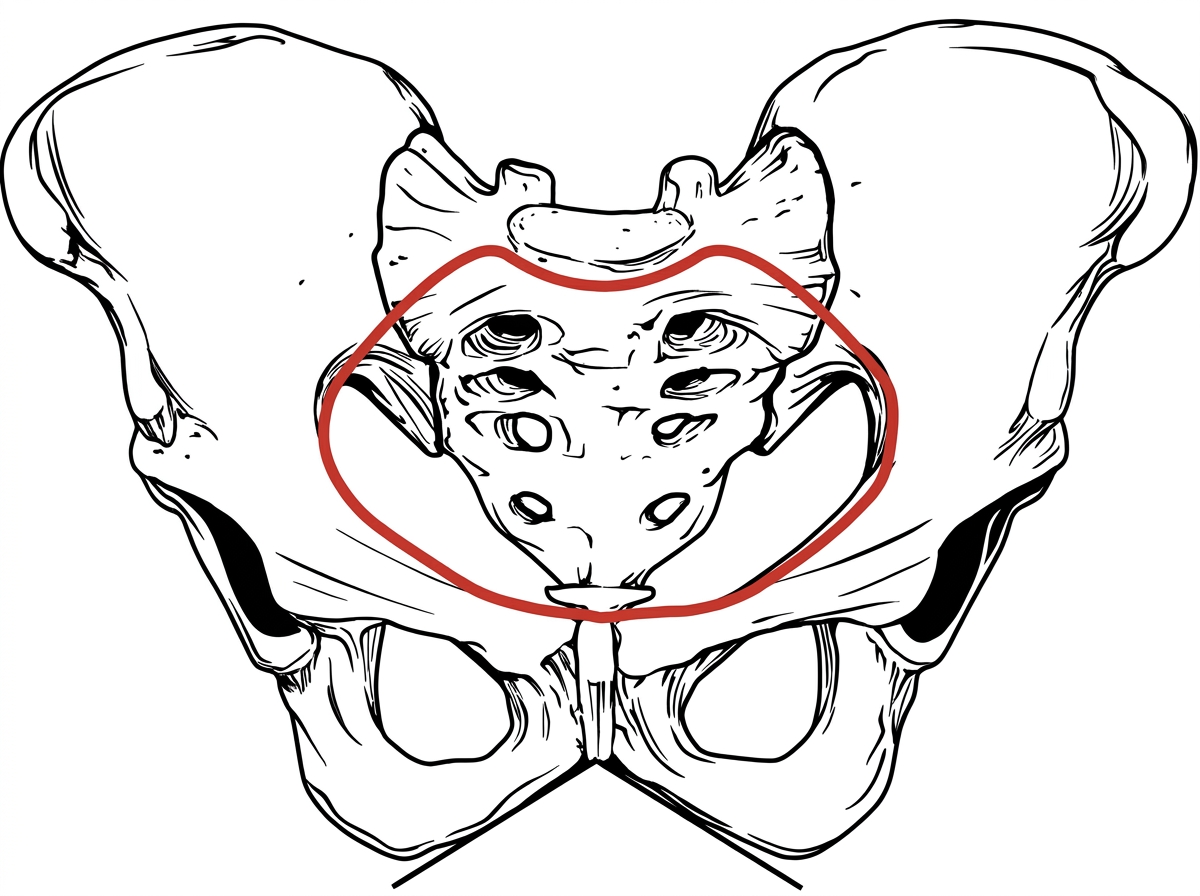
Identify the pelvis type given below.
Identify the type of pelvis in the given image.
Which lymph node is most commonly involved in prostate cancer?
Match the following anatomical structures with their correct image labels: 1. Seminal vesicles 2. Ureter 3. Prostate 4. Vas deferens
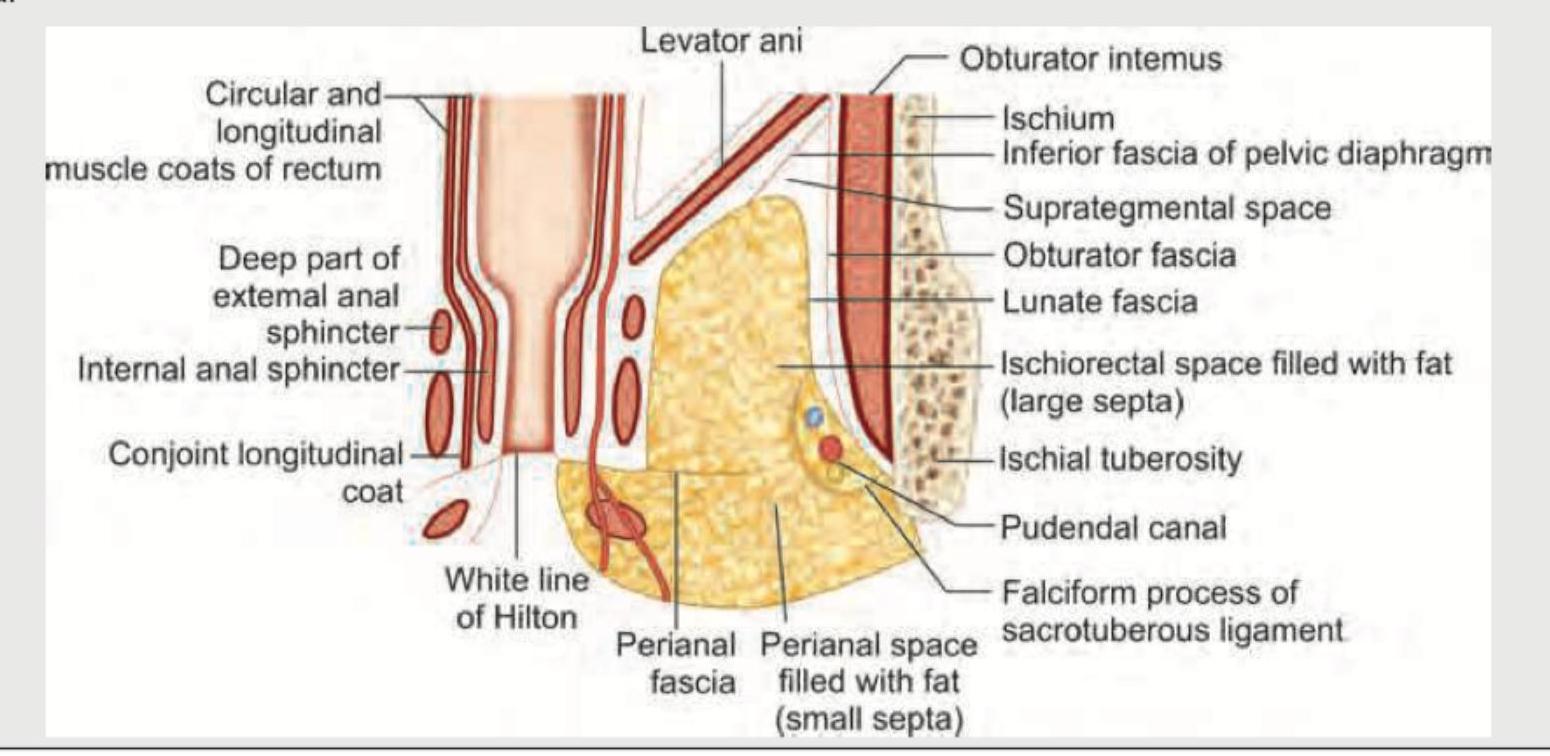
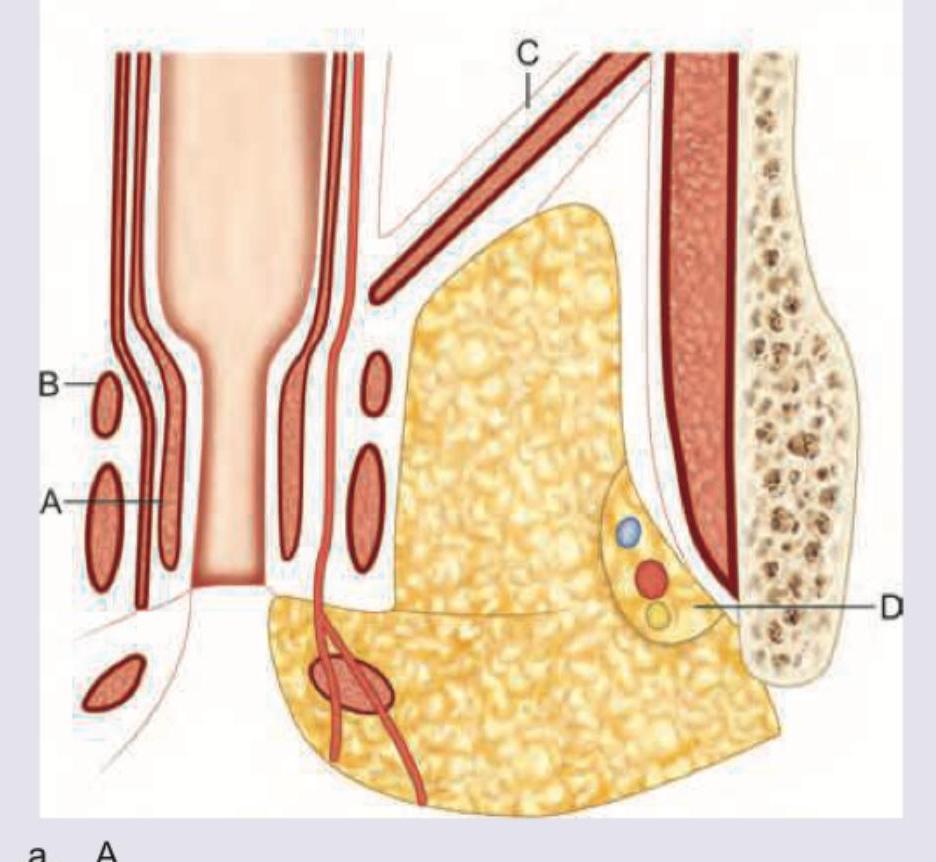
Identify the structure correctly labeled in the given image.
Identify the urogenital diaphragm in the image given below:
Gland of Cloquet is :
Opening of Bartholin's duct is in the :
Blood supply to the uterus comes from which of the following arteries ? 1. Ovarian artery 2. Vaginal artery 3. Uterine artery 4. Inferior vesical artery Select the correct answer using the code given below :
Which of the following set of muscles collectively form the muscle 'Levator Ani' that forms the pelvic floor ? 1. Puborectalis 2. Pubococcygeus 3. Sacrococcygeus 4. Iliococcygeus Select the correct answer using the code given below :
Practice by Chapter
Pelvic Walls and Floor
Practice Questions
Pelvic Viscera
Practice Questions
Urogenital Organs
Practice Questions
Pelvic Vasculature
Practice Questions
Pelvic Innervation
Practice Questions
Male Perineum
Practice Questions
Female Perineum
Practice Questions
Pelvic Lymphatics
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Gender Differences in Pelvic Anatomy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app