
Pelvis and Perineum — MCQs

On this page
What is the ratio of the length of the cervix to that of the corpus of the uterus in an adult woman?
Carcinoma of the prostate commonly metastasizes to the vertebrae, which of the following is the primary reason for this predilection?
Maximum number of mucosal folds are found in which part of the fallopian tube?
Which statement best describes the relationship of the cervix and vagina to surrounding structures?
A 45-year-old man presents after a violent car crash with a perineal 'straddle' injury. An MRI shows extravasating urine and blood from a torn bulbar urethra within the superficial perineal cleft. Which of the following fasciae define the boundaries of this space?
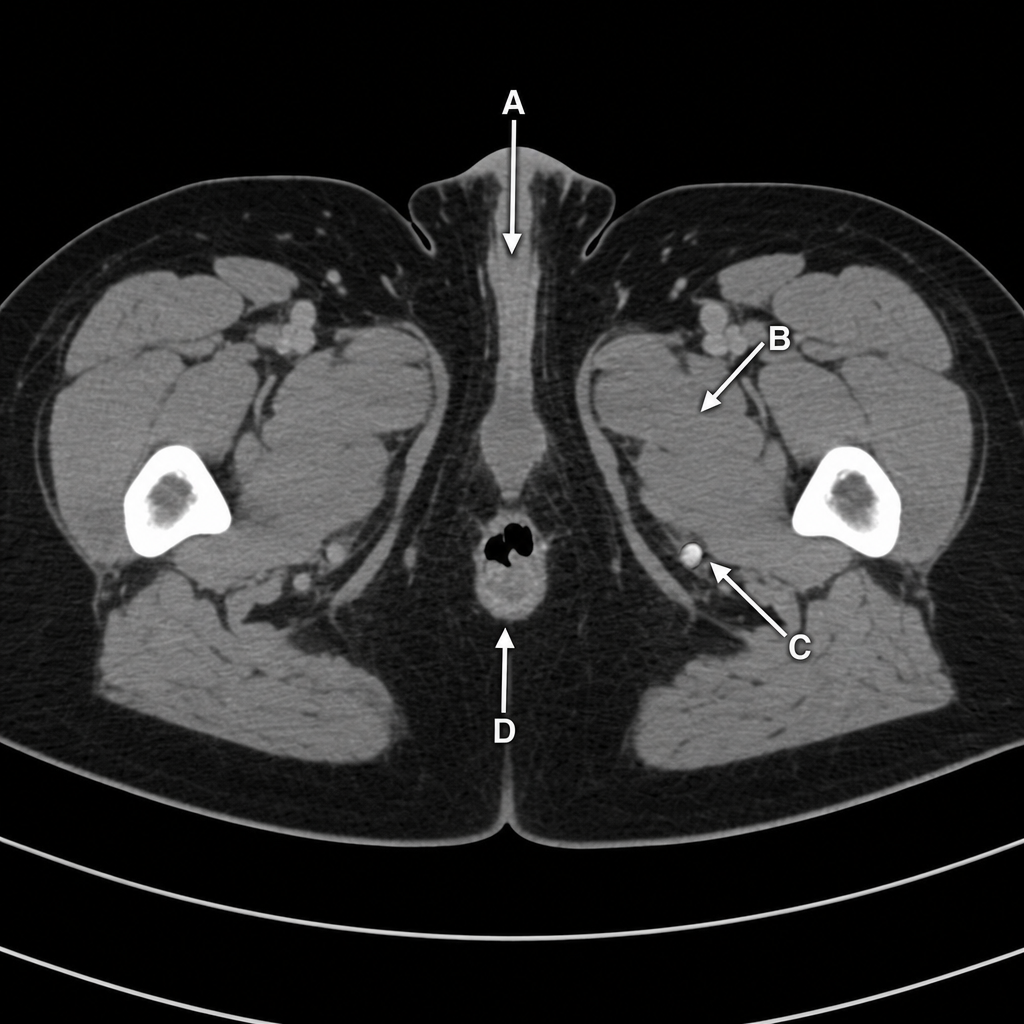
Which structure, shown in a computed tomography scan of the female perineum and pelvis, is innervated by the nerve passing through both the greater and lesser sciatic foramina?
All are components of the urogenital diaphragm except?
A 55-year-old woman complains of fecal incontinence. The most likely contributing factor to such a problem is atrophy, paralysis, or dysfunction of which of the following structures?
What is the narrowest part of the male urethra?
A 19-year-old male sustained an abdominal injury in an accident. Lesions to the fibers in the nervi erigentes lead to the loss of which of the following functions?
Practice by Chapter
Pelvic Walls and Floor
Practice Questions
Pelvic Viscera
Practice Questions
Urogenital Organs
Practice Questions
Pelvic Vasculature
Practice Questions
Pelvic Innervation
Practice Questions
Male Perineum
Practice Questions
Female Perineum
Practice Questions
Pelvic Lymphatics
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Gender Differences in Pelvic Anatomy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app