
Pelvis and Perineum — MCQs

On this page
Which of the following statements is NOT true concerning the dentate line of the anal canal?
Which of the following statements about the prostatic venous plexus is incorrect?
All of the following structures pass through the lesser sciatic foramen, EXCEPT?
The superior and inferior vesicular arteries are branches of which artery?
Which of the following is not a muscular support of the uterus?
Which of the following is NOT a muscle forming the floor of the pelvis?
Which statement best describes the pelvic viscera?
A neurosurgeon performs a surgical resection of a rare meningeal tumor in the sacral region. He attempts to avoid injury to the nerve that arises from the lumbosacral plexus and remains within the abdominal or pelvic cavity. To which of the following nerves should he pay particular attention?
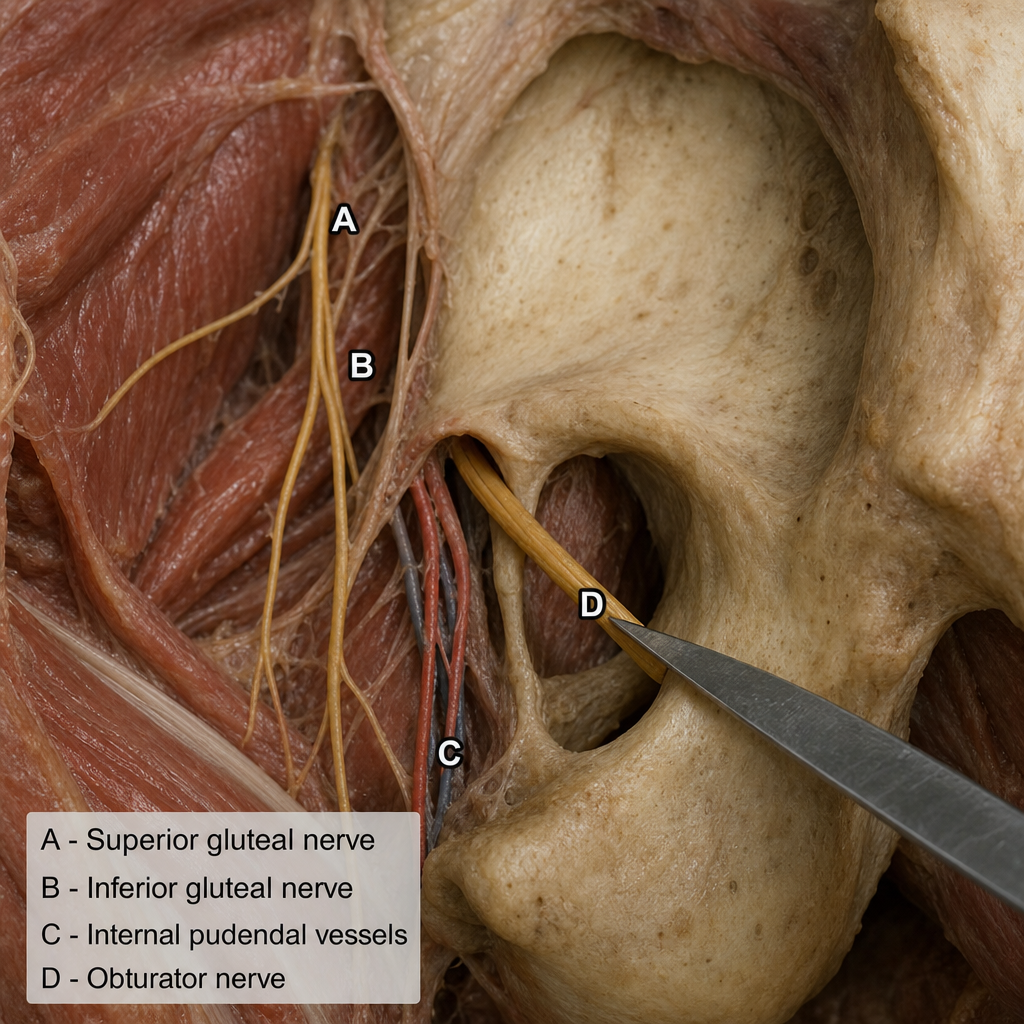
A knife wound to the obturator canal at the superior margin of the obturator foramen might injure which structure?
The parasympathetic nerves that produce uterine inhibition and vasodilatation of uterine vessels arise from which segments of the vertebrae?
Practice by Chapter
Pelvic Walls and Floor
Practice Questions
Pelvic Viscera
Practice Questions
Urogenital Organs
Practice Questions
Pelvic Vasculature
Practice Questions
Pelvic Innervation
Practice Questions
Male Perineum
Practice Questions
Female Perineum
Practice Questions
Pelvic Lymphatics
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Gender Differences in Pelvic Anatomy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app