
Pelvis and Perineum — MCQs

On this page
Which of the following does not form the triradiate ligament of the uterus?
Which of the following muscles attaches to the perineal body?
Which of the following is NOT an anatomical feature of the prostatic urethra?
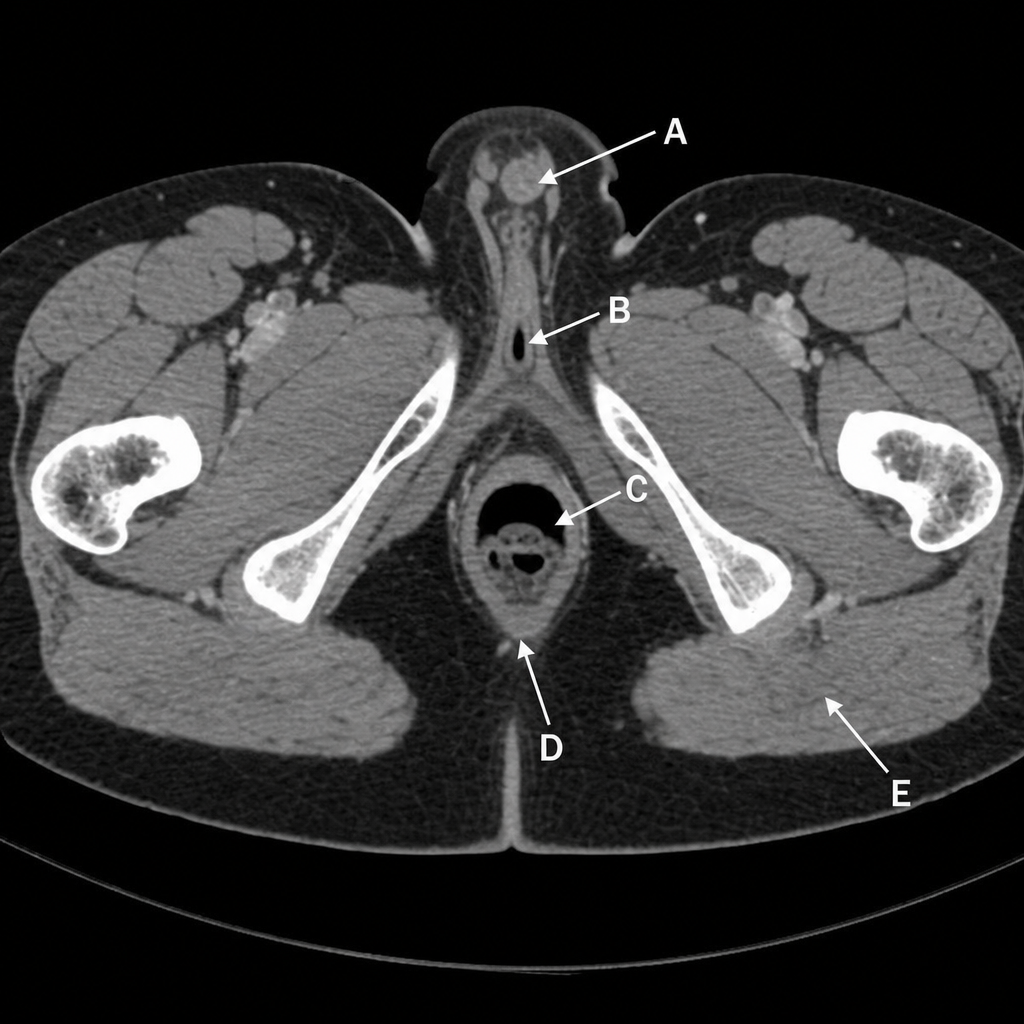
A CT scan of the male perineum and pelvis is provided. Which labeled structure is characterized by Houston's valve or fold and has its upper-portion venous blood drained by the portal venous system?
Which ligament is pierced by the needle to reach the pudendal nerve during a pudendal nerve block?
Ovarian pathology is referred to which anatomical region?
What are the cardinal ligaments of the uterus?
Which of the following does NOT form the lateral wall of the ischiorectal fossa?
Which of the following statements regarding the levator ani muscle is FALSE?
Smegma is secreted by which gland?
Practice by Chapter
Pelvic Walls and Floor
Practice Questions
Pelvic Viscera
Practice Questions
Urogenital Organs
Practice Questions
Pelvic Vasculature
Practice Questions
Pelvic Innervation
Practice Questions
Male Perineum
Practice Questions
Female Perineum
Practice Questions
Pelvic Lymphatics
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Gender Differences in Pelvic Anatomy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app