
Neck — MCQs

On this page
The danger space in front of the prevertebral fascia extends till which anatomical landmark?
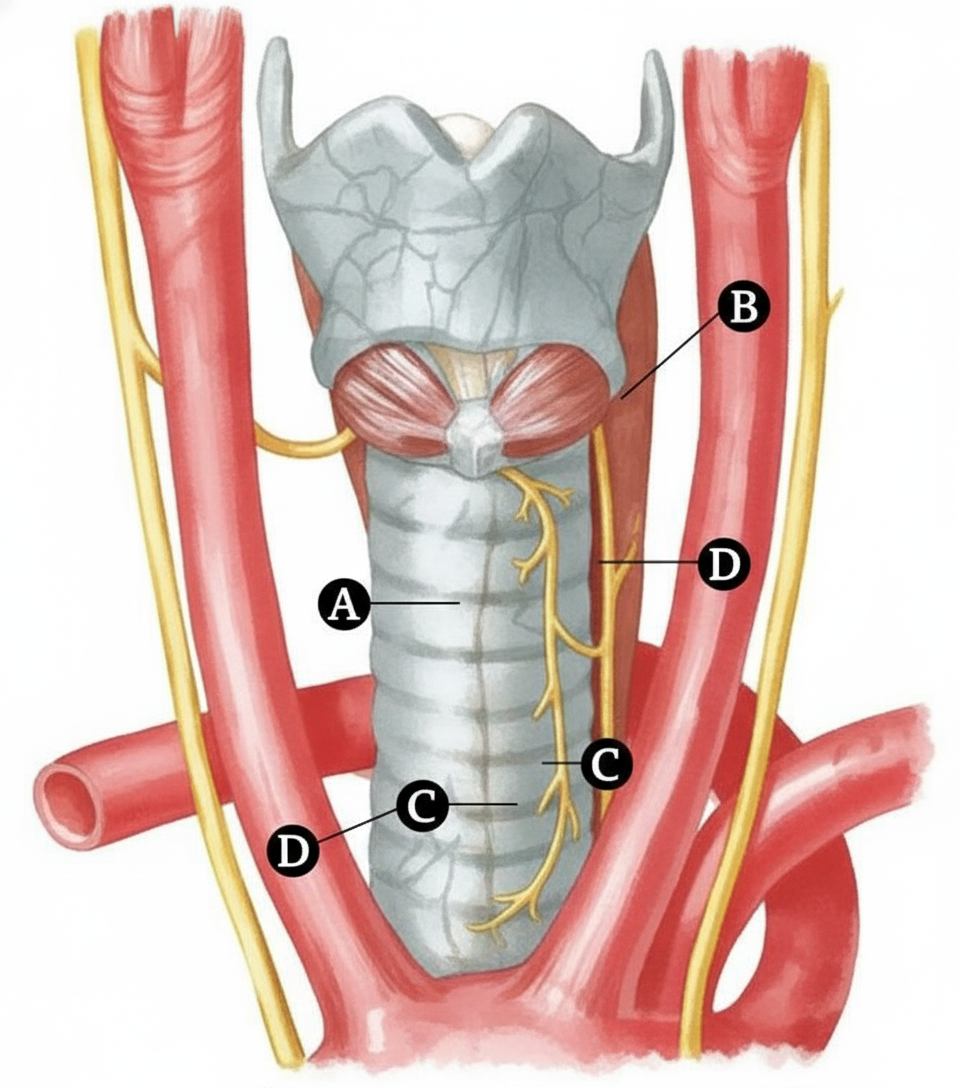
Different nerves are marked in the given diagram. Which of the following nerves supplies the posterior cricoarytenoid muscle?
All of the following are true about the phrenic nerve, except?
All of the following are branches of the subclavian artery except:
The suprasternal space contains all of the following structures except which one?
Which level of lymph nodes are the pretracheal and paratracheal lymph nodes?
Which of the following statements about the subclavian artery is FALSE?
Which nerve winds around the subclavian artery?
Which of the following actions is performed by the platysma muscle?
A 21-year-old woman presents with a neck swelling, diagnosed as an infection within the carotid sheath. Which of the following structures would be damaged?
Practice by Chapter
Cervical Fascia
Practice Questions
Triangles of the Neck
Practice Questions
Deep Structures of the Neck
Practice Questions
Thyroid and Parathyroid Glands
Practice Questions
Vasculature of the Neck
Practice Questions
Lymphatic Drainage
Practice Questions
Cervical Plexus
Practice Questions
Root of the Neck
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Surface Anatomy of the Neck
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app