
Neck — MCQs

On this page
Which muscles are tensors of the vocal cords?
Which of the following hyoid muscles is an important landmark in both the anterior and posterior triangles of the neck?
Following a surgical procedure on the right side of the neck, a patient cannot raise their right arm above the horizontal position and cannot shrug their right shoulder. Which of the following nerves was injured?
The loop of Gallen is a type of anastomosis in the larynx?
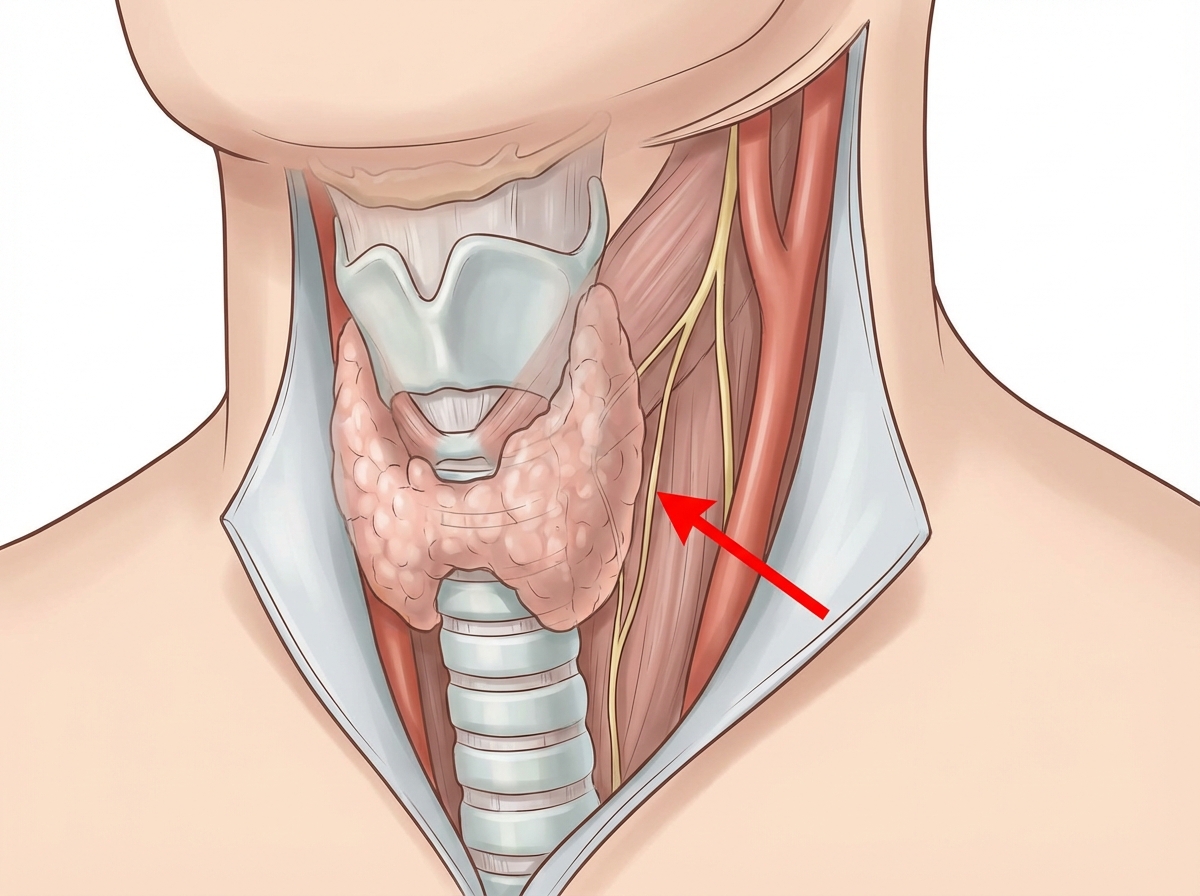
Identify the nerve indicated by the arrow, which is important during surgery of the overlying organ.
The spinal part of the accessory nerve supplies which of the following muscles?
A 31-year-old man sustained a shrapnel wound in the neck. On examination, it was noticed that when he blew his nose or sneezed, the skin above the right clavicle bulged upward. Which of the following best explains this phenomenon?
What is the narrowest part of the pediatric airway?
Which of the following group of lymph nodes are known as 'delphic nodes'?
The recurrent laryngeal nerve has a close anatomical relationship with which of the following structures?
Practice by Chapter
Cervical Fascia
Practice Questions
Triangles of the Neck
Practice Questions
Deep Structures of the Neck
Practice Questions
Thyroid and Parathyroid Glands
Practice Questions
Vasculature of the Neck
Practice Questions
Lymphatic Drainage
Practice Questions
Cervical Plexus
Practice Questions
Root of the Neck
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Surface Anatomy of the Neck
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app