
Neck — MCQs

On this page
A 33-year-old male patient complains of severe pain when he tries to turn his neck. The physician realizes that the problem is in his pivot (trochoid) joint. Which of the following joints would most likely be examined?
All of the following nerves may be injured during the excision of the submandibular salivary gland except:
What is the most common site of the internal opening of a branchial fistula?
Which of the following statements is true about the atlanto-axial joint?
A baby can breathe and suck simultaneously. This is facilitated by which anatomical feature?
The submandibular gland is divided into superficial and deep parts by which muscle?
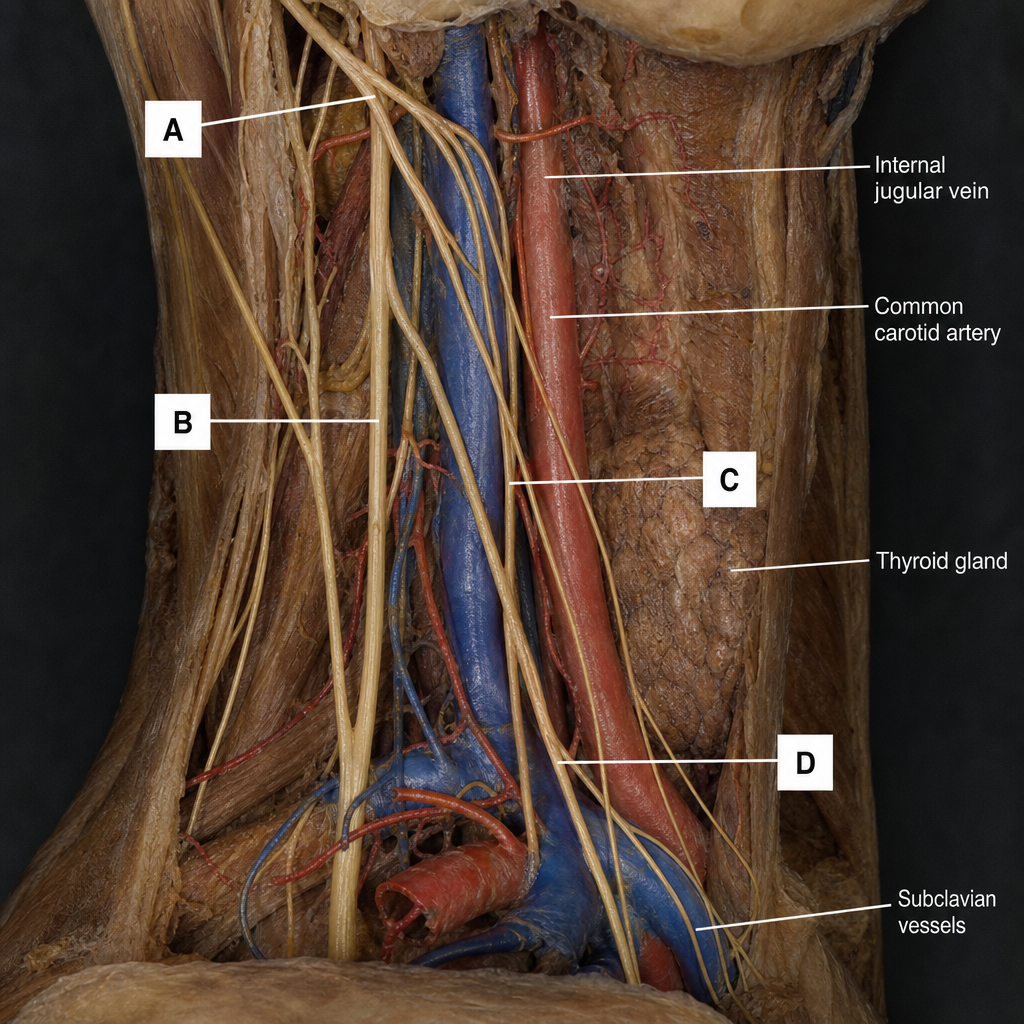
Which of the marked structures A, B, C, or D in the illustration represents the vagus nerve?
Which of the following structures is NOT present on the medial surface of the submandibular gland?
Which of the following is an extrinsic membrane of the larynx?
Which of the following statements about the larynx is false?
Practice by Chapter
Cervical Fascia
Practice Questions
Triangles of the Neck
Practice Questions
Deep Structures of the Neck
Practice Questions
Thyroid and Parathyroid Glands
Practice Questions
Vasculature of the Neck
Practice Questions
Lymphatic Drainage
Practice Questions
Cervical Plexus
Practice Questions
Root of the Neck
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Surface Anatomy of the Neck
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app