
Neck — MCQs

On this page
A patient presents with swelling in the neck, difficulty swallowing, and a hoarse voice. Which nerve is most likely involved?
Which structure forms the superior (anterior) boundary of the carotid triangle?
A patient with a stab wound to the neck presents with difficulty breathing and hoarseness. Which structure is most likely to be injured?
Which artery supplies the superficial structures of the head and neck region and is a branch of the common carotid artery?
A 65-year-old male presents with difficulty swallowing and a hoarse voice. Imaging reveals a mass at the level of the cricoid cartilage. Which nerve is most likely to be compressed?
A surgeon accidentally lacerates a nerve close to the angle of the mandible during a submandibular gland excision. Which nerve is at risk in this situation?
Which cervical vertebra is known as the 'vertebra prominens' because of its distinctive spinous process?
During an emergency tracheotomy, which anatomical landmarks should be identified to ensure the correct placement of the incision?
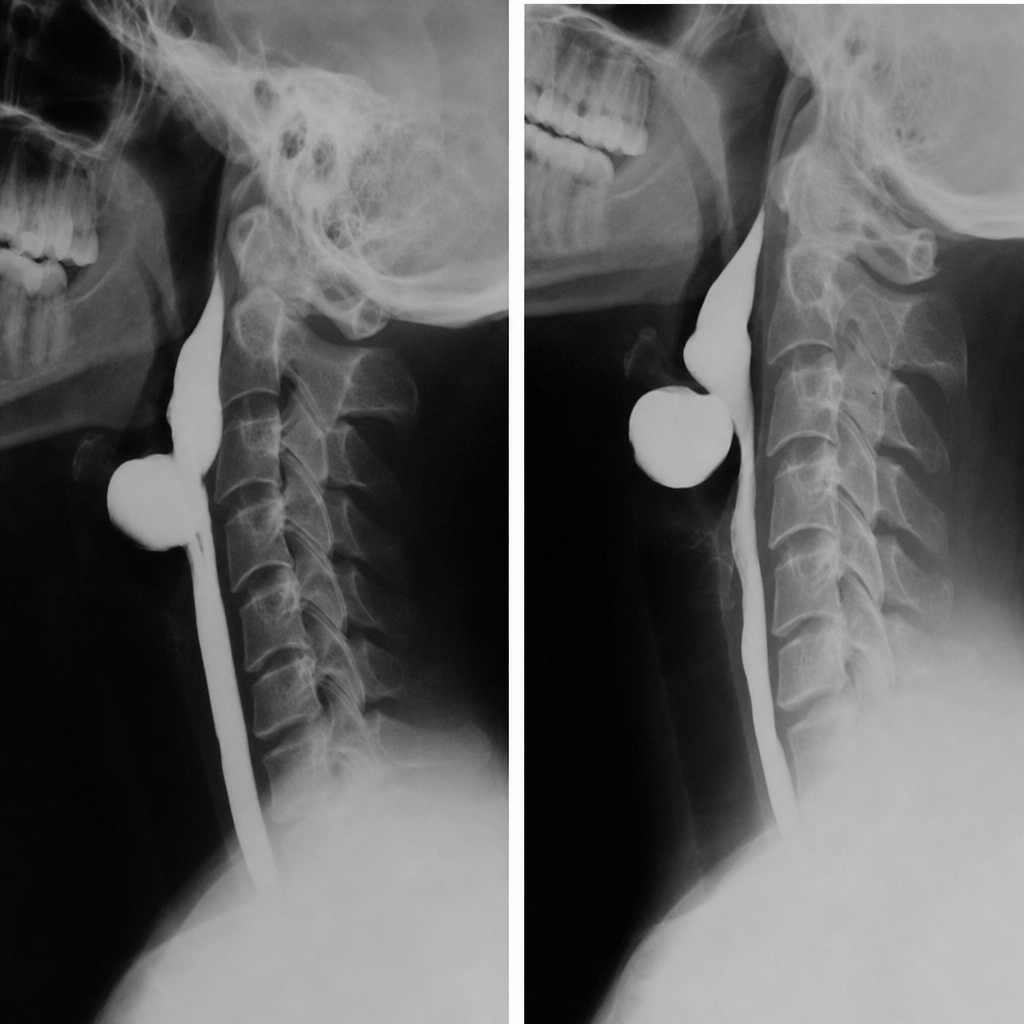
The most common site of origin of the diverticulum of the pharynx seen in the barium swallow given below is
Which of the following is the PRIMARY anatomical location of the parathyroid glands?
Practice by Chapter
Cervical Fascia
Practice Questions
Triangles of the Neck
Practice Questions
Deep Structures of the Neck
Practice Questions
Thyroid and Parathyroid Glands
Practice Questions
Vasculature of the Neck
Practice Questions
Lymphatic Drainage
Practice Questions
Cervical Plexus
Practice Questions
Root of the Neck
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Surface Anatomy of the Neck
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app