
Neck — MCQs

On this page
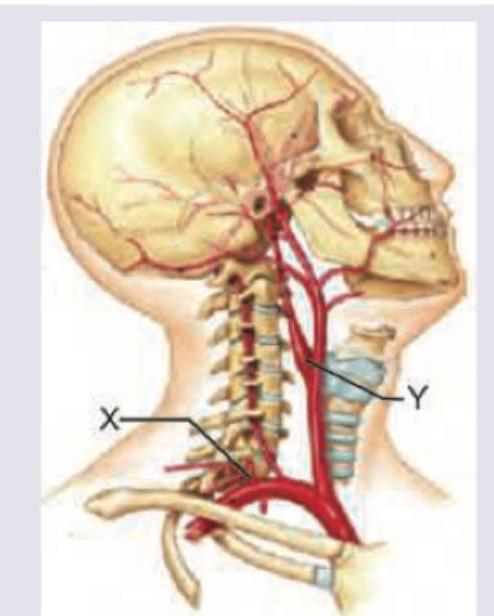
Which structures are marked as $X$ and $Y$ ?
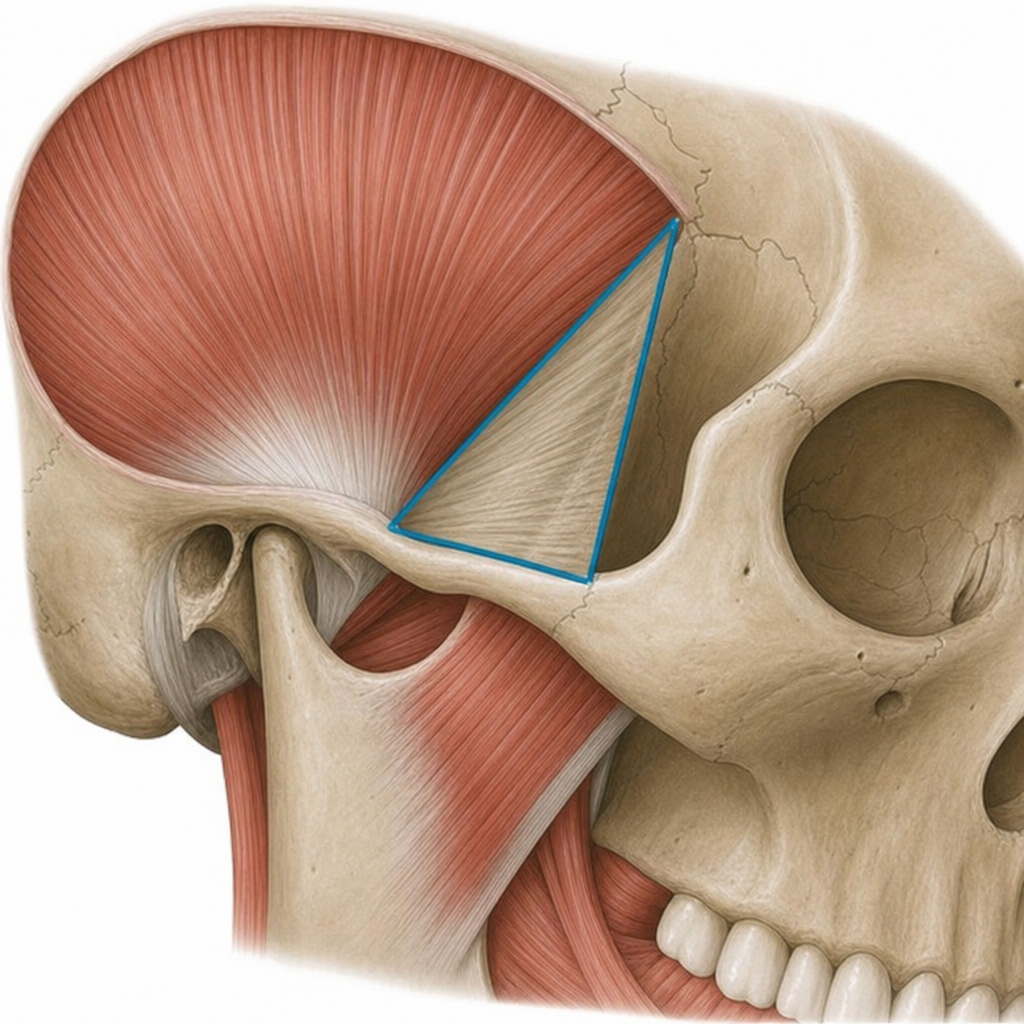
Identify the triangle shown in the figure below:
Identify the structure marked as $X$ below:
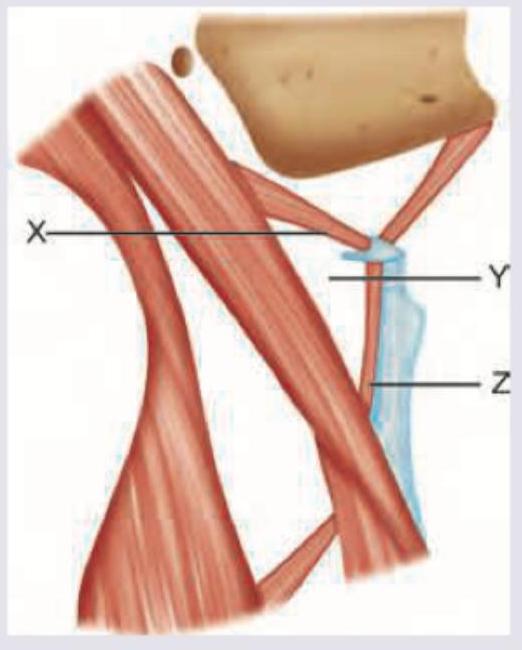
Identify the anatomical structures-X, Y, Z of the neck depicted below in that order: (APPG 2015)
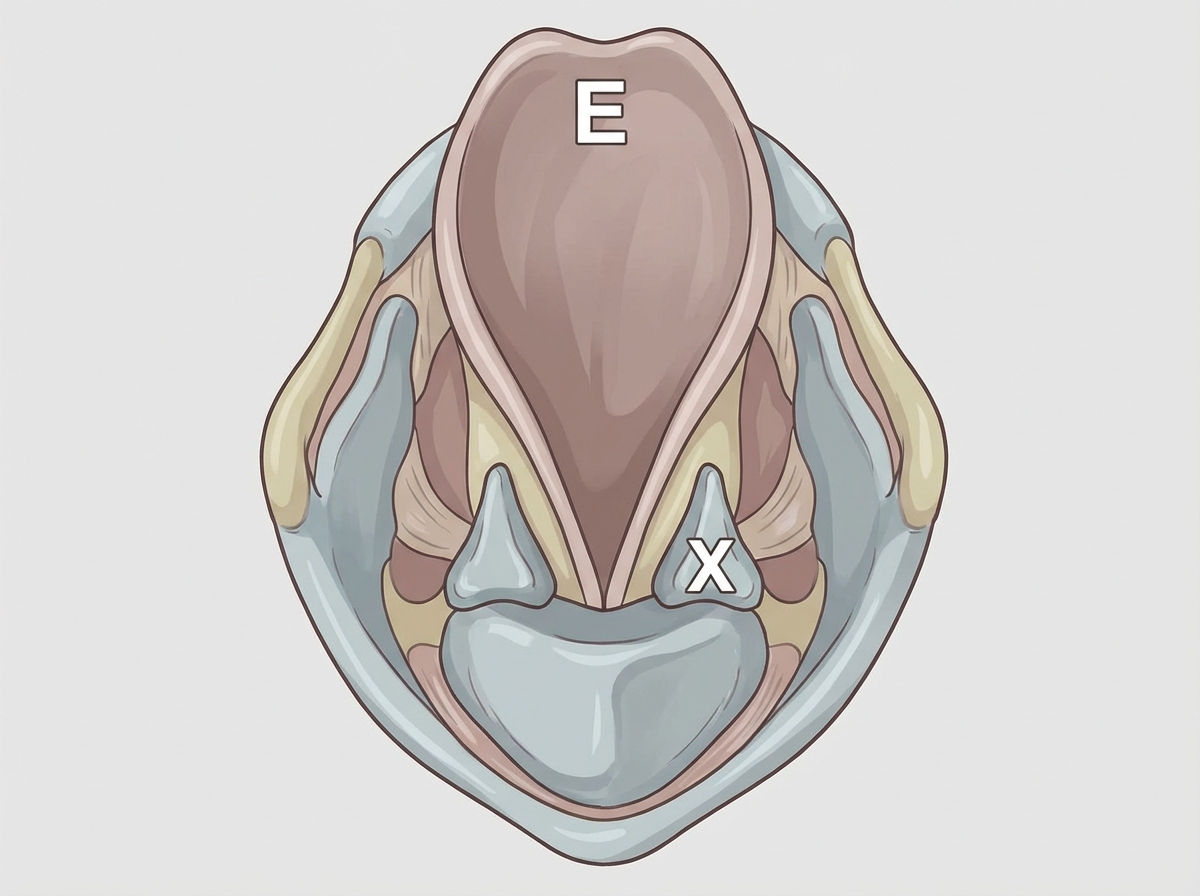
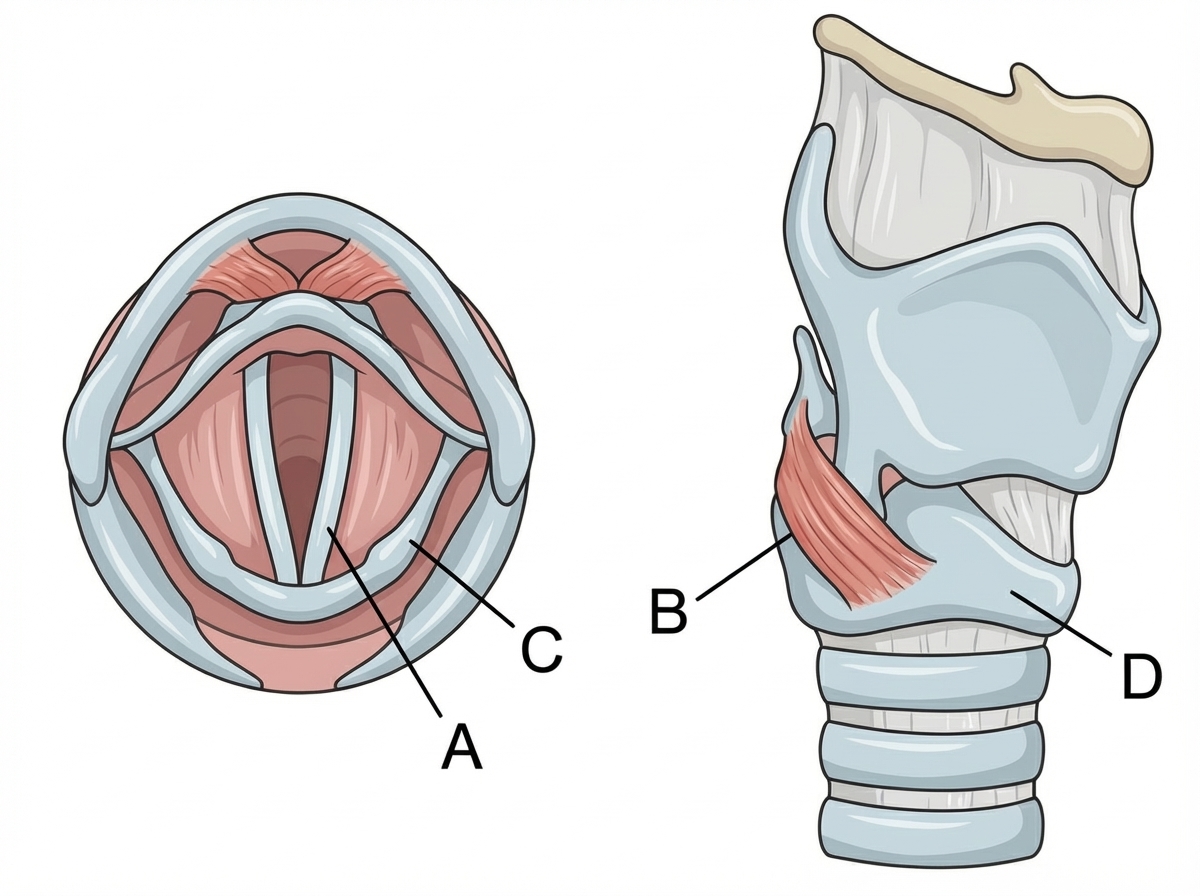
The superior and posterior views of the larynx are shown below. Which label identifies the abductor of the vocal cords?
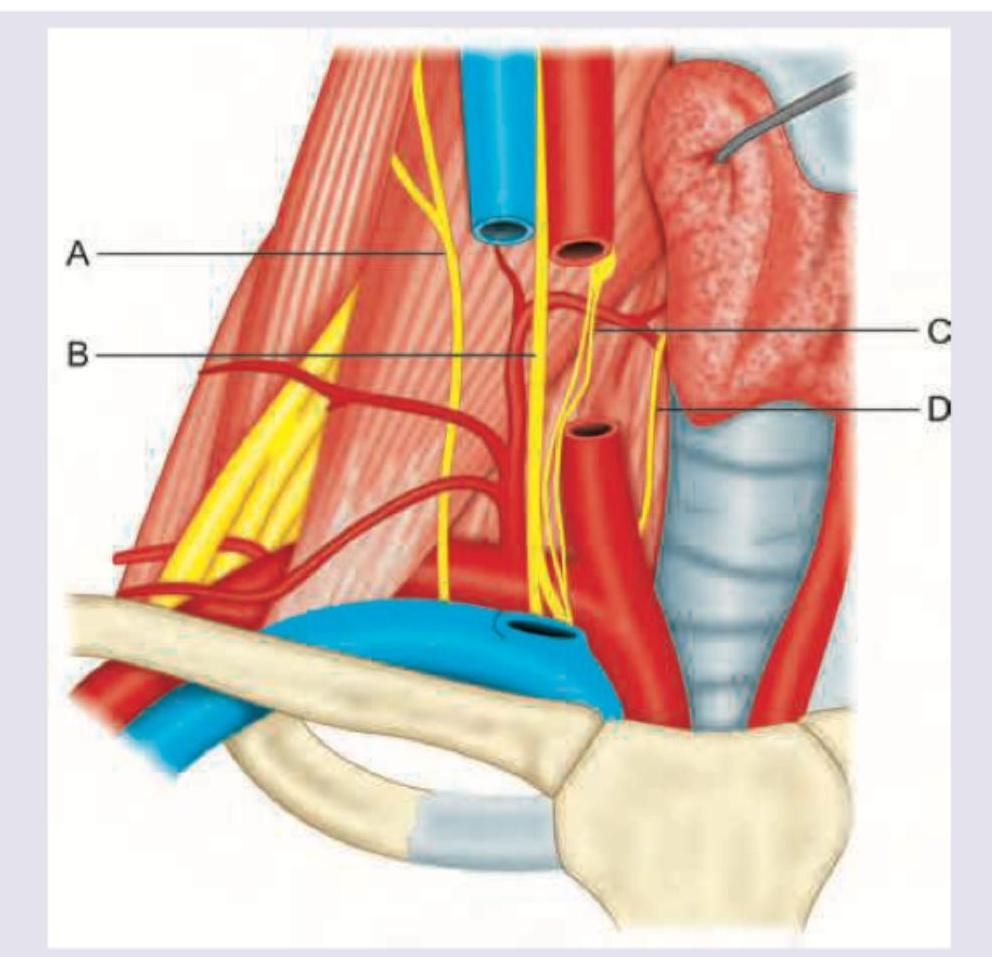
In this diagram, identify the structure whose paralysis causes decrease in respiratory movements: (AIIMS May 2016)
Which structure passes through the area marked in red? (AIIMS May 2018)
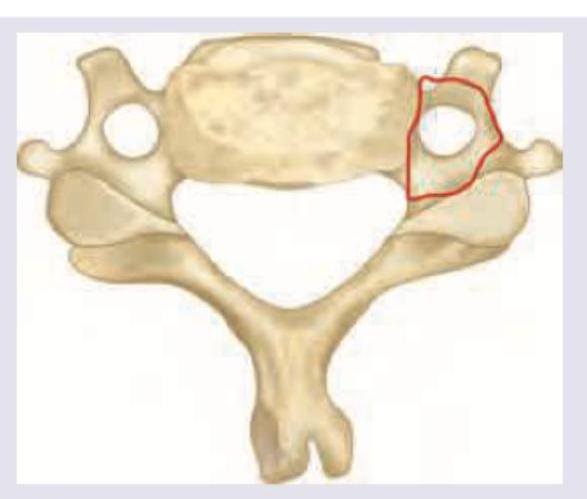
8. Ans. (a) Quadrangular membrane

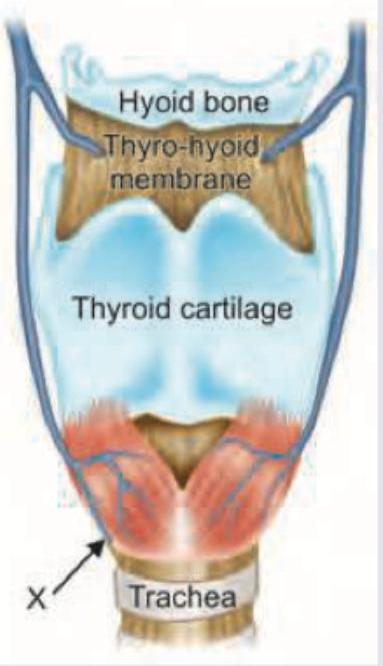
What does the marking X represent? (DNB Pattern 2018)

The marking X represents which muscle? (DNB Pattern 2018)
Practice by Chapter
Cervical Fascia
Practice Questions
Triangles of the Neck
Practice Questions
Deep Structures of the Neck
Practice Questions
Thyroid and Parathyroid Glands
Practice Questions
Vasculature of the Neck
Practice Questions
Lymphatic Drainage
Practice Questions
Cervical Plexus
Practice Questions
Root of the Neck
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Surface Anatomy of the Neck
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app