
Neck — MCQs

On this page
The tonsillar fossa is bounded anteriorly by which structure?
Which is the narrowest part of the adult laryngeal airway?
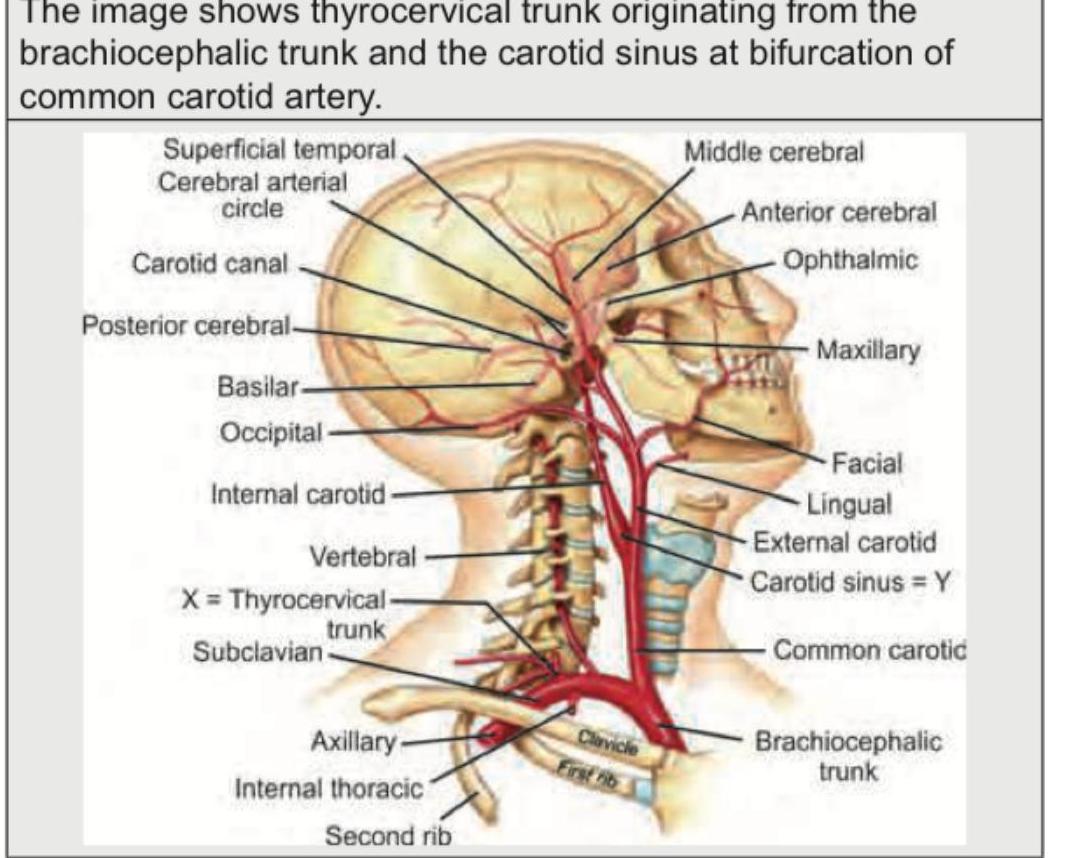
Identify the structure marked as 'X' in the image below
A patient presents with loss of sensation on the posterior surface of the ear along with a lesion. Which structure is most likely involved?
Identify the level of lymph nodes indicated in the marked region of the neck in the given anatomical image.
A 35-year-old man presents to the emergency department with a complaint of food stuck in his throat. On examination, a bone is seen in the left piriform recess. Which of the following is most likely to be impaired?
A middle-aged lady choked while eating fish and has associated symptoms of coughing, hoarseness of voice, and a foreign body sensation in the throat. On examination, the pyriform fossa is found to be inflamed. Which of the following nerves supplies this region?
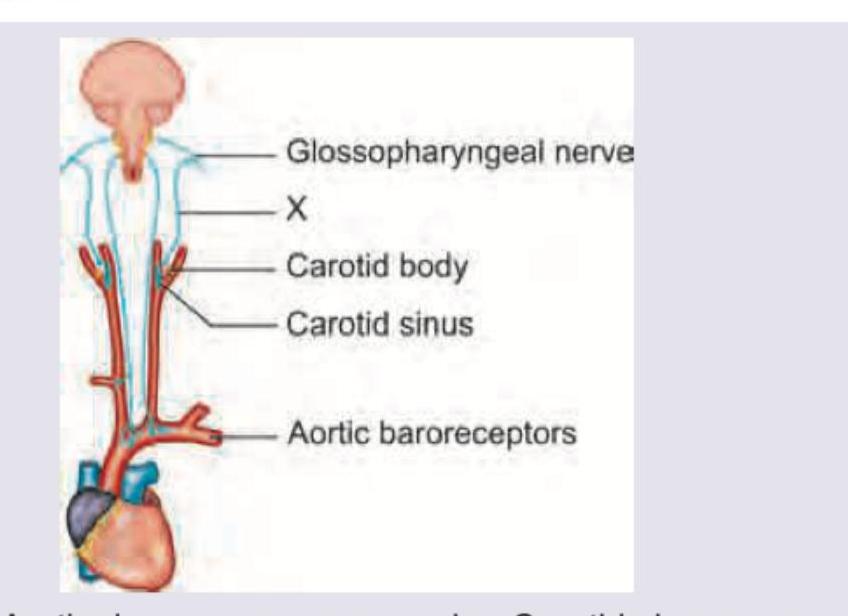
Which nerve marked as X innervates the carotid sinus?
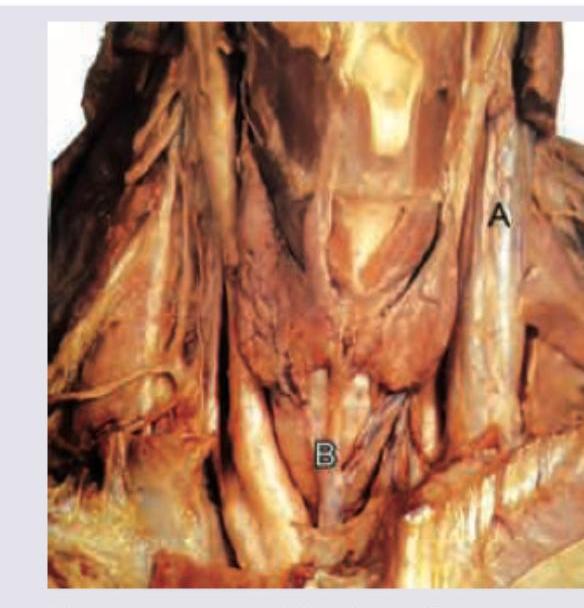
Identify the marked parts in the given image.
The following image shows:
Practice by Chapter
Cervical Fascia
Practice Questions
Triangles of the Neck
Practice Questions
Deep Structures of the Neck
Practice Questions
Thyroid and Parathyroid Glands
Practice Questions
Vasculature of the Neck
Practice Questions
Lymphatic Drainage
Practice Questions
Cervical Plexus
Practice Questions
Root of the Neck
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Surface Anatomy of the Neck
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app