
Neck — MCQs

On this page
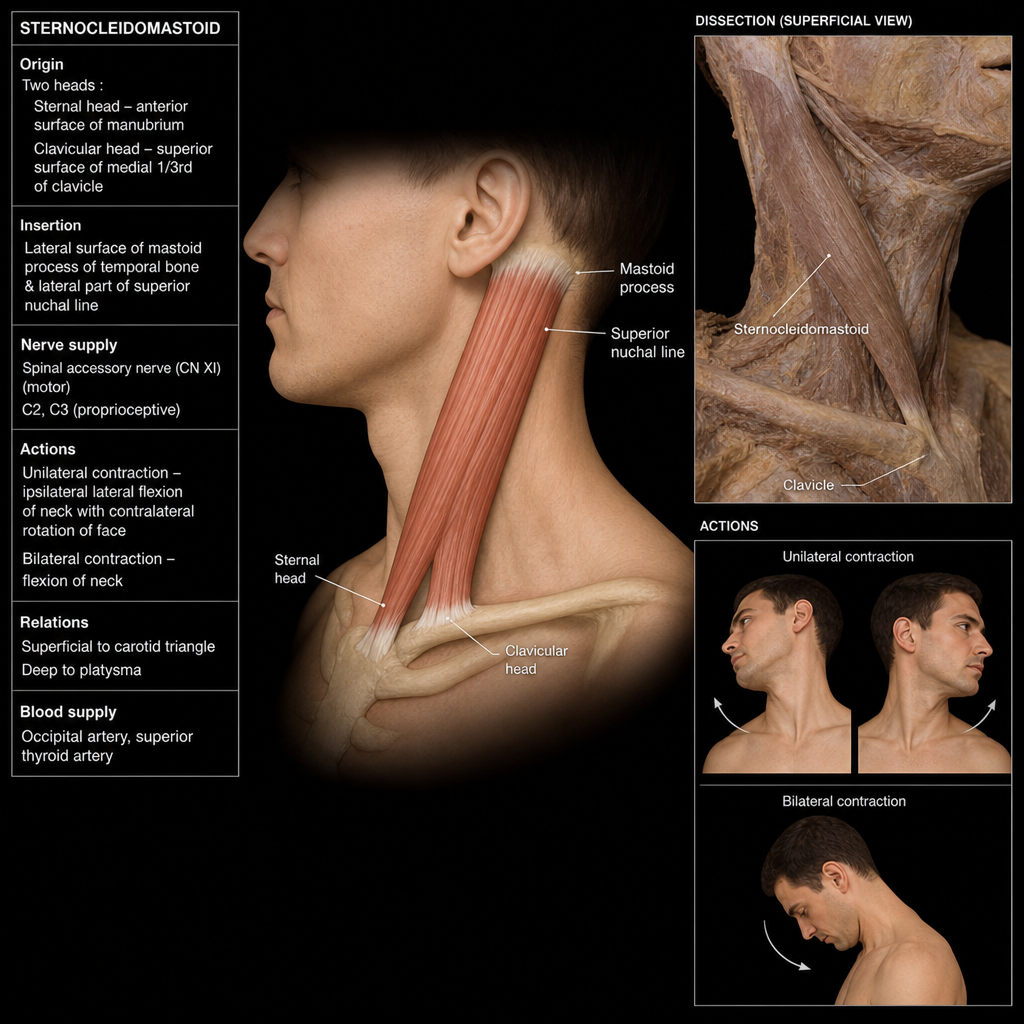
Which of the following statements are true about the sternocleidomastoid muscle?
The superior thyroid artery originates from which of the following arteries?
Which of the following statements is NOT true regarding the deep cervical lymph nodes?
Which vein collects blood from the common facial vein?
Which muscle is responsible for the change in pitch of sound?
What is the usual number of parathyroid glands in a human?
What is the most common site of subclavian artery stenosis?
The inferior thyroid artery arises from which of the following?
What is true regarding the lymphatic drainage of the neck?
Which of the following statements regarding thyroidectomy is incorrect?
Practice by Chapter
Cervical Fascia
Practice Questions
Triangles of the Neck
Practice Questions
Deep Structures of the Neck
Practice Questions
Thyroid and Parathyroid Glands
Practice Questions
Vasculature of the Neck
Practice Questions
Lymphatic Drainage
Practice Questions
Cervical Plexus
Practice Questions
Root of the Neck
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Surface Anatomy of the Neck
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app