
Neck — MCQs

On this page
The recurrent laryngeal nerve supplies all laryngeal muscles except which one?
What is the distance from the central incisor to the cricopharyngeal sphincter?
Cervical esophagus receives its arterial supply from which artery?
A 55-year old male presents for evaluation of a lesion on his lower lip for the past year. He is employed as a landscaper and reports infrequent use of sun protection. He denies any pertinent medical history. Physical examination reveals a 5 mm erythematous, ulcerative nodule located within the vermilion of the right lateral aspect of the lower lip. Biopsy confirms the presence of invasive squamous cell carcinoma and the patient is referred for Mohs micrographic surgical excision. Which of the following lymph nodes would be most critical to evaluate for metastasis?
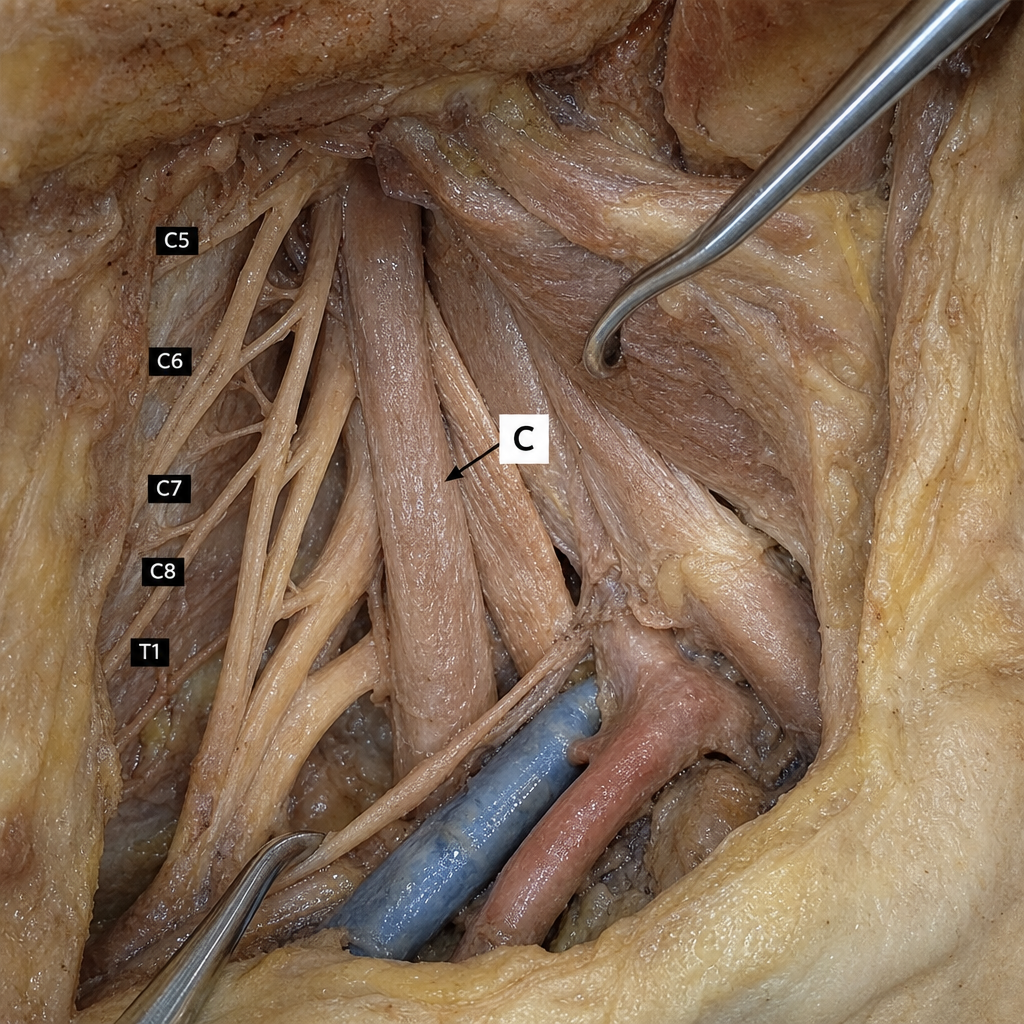
Structure lying at marker C?
A 37-year-old man presents with a neck injury. Radiographic imaging reveals a crushed C2 vertebra. Which of the following structures would remain intact following this injury?
Exposure of the left subclavian artery by a supraclavicular approach does NOT require cutting of which muscle?
A 56-year-old woman has undergone a complete thyroidectomy. Post-operatively, hoarseness of voice is noted, persisting for 3 weeks. Examination reveals a permanently adducted vocal fold on the right side. Surgical trauma to the innervation of which of the following muscles is most likely responsible for the position of the right vocal fold?
All of the following are true about branchial cysts except?
All of the following form the boundaries of the digastric triangle except?
Practice by Chapter
Cervical Fascia
Practice Questions
Triangles of the Neck
Practice Questions
Deep Structures of the Neck
Practice Questions
Thyroid and Parathyroid Glands
Practice Questions
Vasculature of the Neck
Practice Questions
Lymphatic Drainage
Practice Questions
Cervical Plexus
Practice Questions
Root of the Neck
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Surface Anatomy of the Neck
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app