
Microscopic Anatomy of Respiratory System — MCQs

In a preterm baby with respiratory distress syndrome, which of the following lipids would be deficient?
The activation of muscarinic receptors in bronchiolar smooth muscle is associated with:
All of the following are features of Lymph node histology except:
Which of the following is a stain for heart failure cells?
Investigation of choice for Posterior urethral valves?
Granuloma is a pathological feature of all, except which of the following?
Which of the following diseases is NOT associated with Anti-Neutrophil Cytoplasmic Antibodies (ANCA)?
The nasopharynx is primarily lined by which type of epithelium?
All cartilage is covered by perichondrium, except
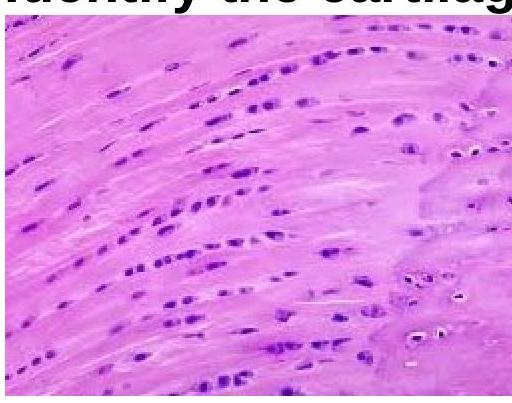
Identify the type of cartilage shown in the image.
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app