
Histology — MCQs

On this page
A 10-year-old boy has sustained a severed radial nerve. Which of the following cells plays a major role in axonal regrowth?
Which of the following karyotyping techniques is performed using fluorescence microscopy?
Purkinje fibres are:
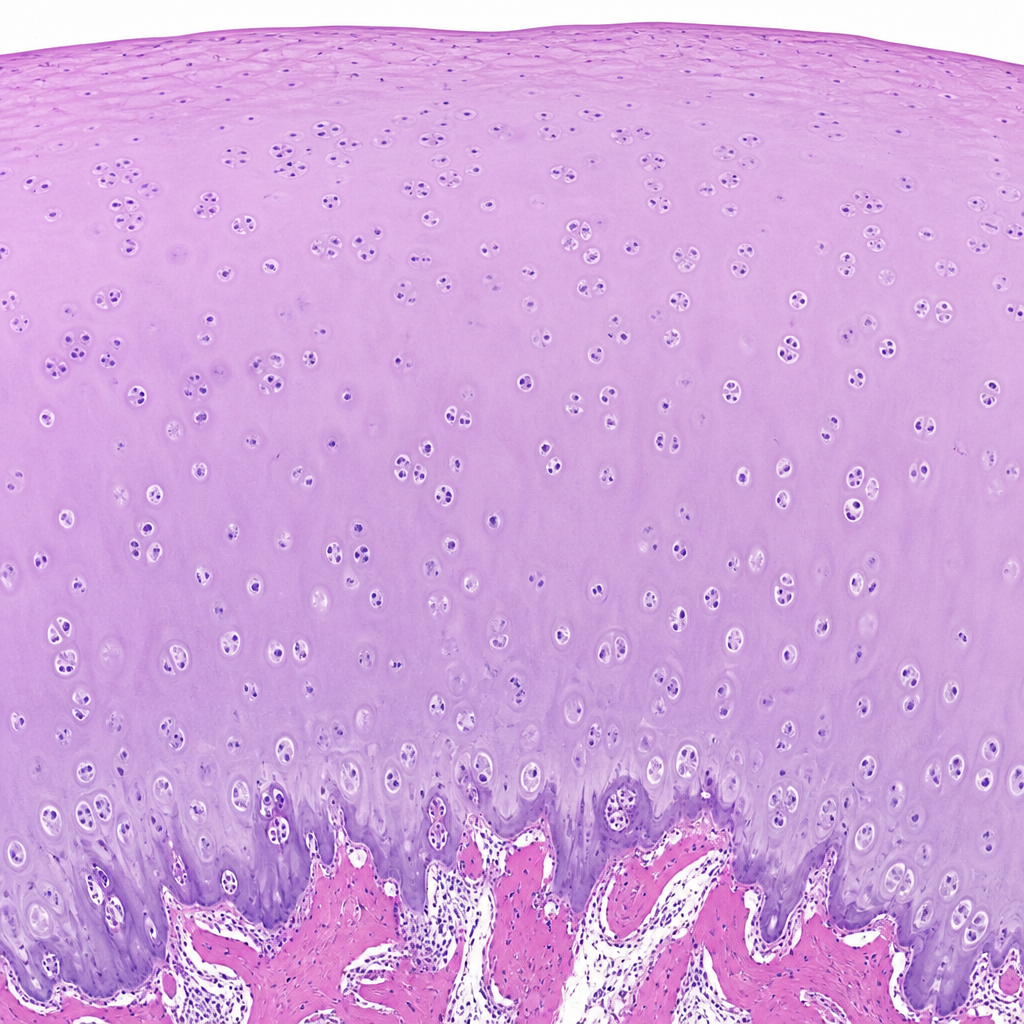
Microscopic examination of the articular surface of a synovial joint demonstrates the following histology representing:
B-cells are dispersed in which part of the spleen?
Which of the following cell types are NOT found in the stomach?
The receptor cells of the olfactory epithelium are?
Lymphocytes are located in each of the following tissues or organs EXCEPT one. What is the exception?
Birbeck granules are seen in the cytoplasm of which of the following cells?
Which of the following is associated with ependymal cells rather than microglial cells?
Practice by Chapter
Basic Tissue Types
Practice Questions
Cell Biology and Organelles
Practice Questions
Epithelial Tissue
Practice Questions
Connective Tissue
Practice Questions
Muscular Tissue
Practice Questions
Nervous Tissue
Practice Questions
Cardiovascular System Histology
Practice Questions
Lymphoid Organs and Immune System
Practice Questions
Endocrine System Histology
Practice Questions
Respiratory System Histology
Practice Questions
Digestive System Histology
Practice Questions
Urinary and Reproductive System Histology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app