
Histology — MCQs

On this page
Where are pneumocytes located?
Submucosal glands are present in which one of the following organs?
Which of the following is NOT a characteristic feature of skeletal muscle?
The pharyngeal tonsil is lined by which type of epithelium?
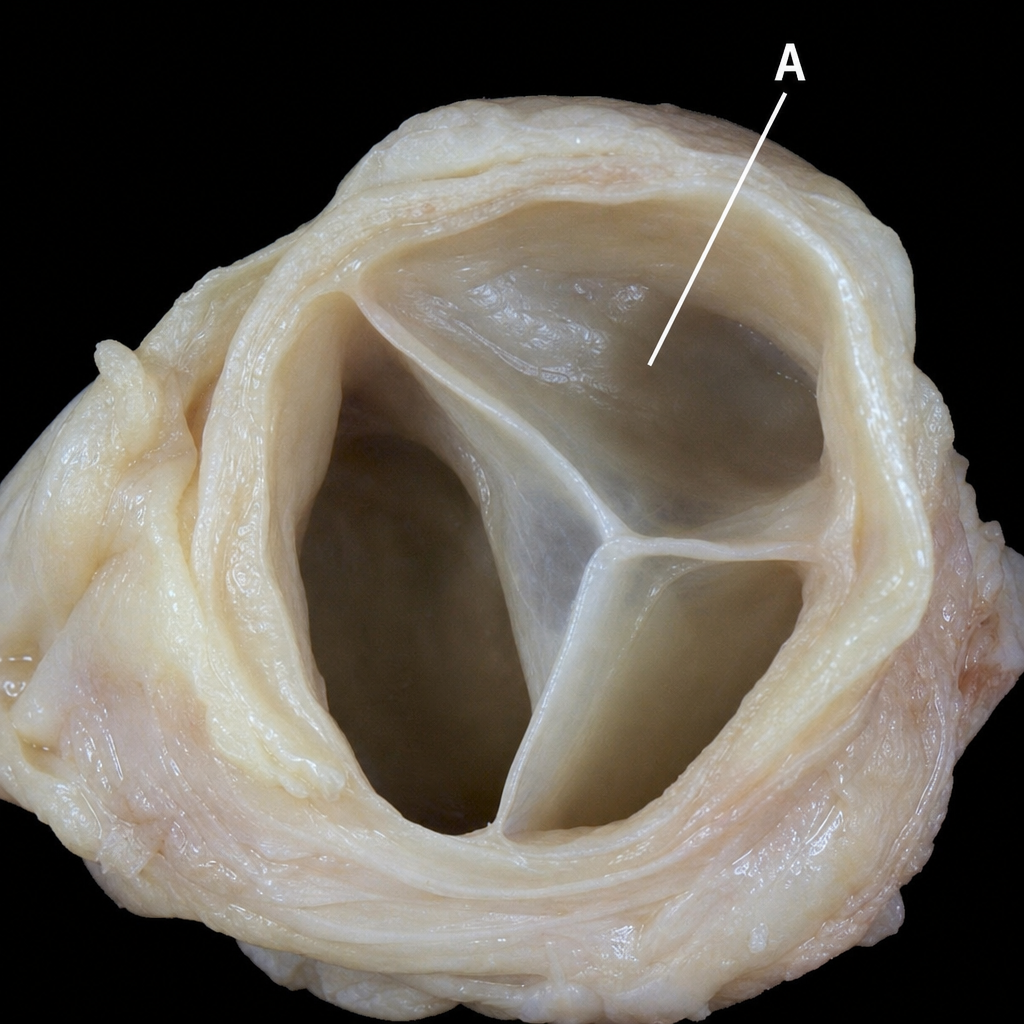
The covering of A is?
Actin is attached to the Z-line by which protein?
The Auerbach plexus is present in which layer of the gastrointestinal tract?
Dust cells can be found in which organ?
Corpora amylacea are found in which gland?
The submandibular gland is:
Practice by Chapter
Basic Tissue Types
Practice Questions
Cell Biology and Organelles
Practice Questions
Epithelial Tissue
Practice Questions
Connective Tissue
Practice Questions
Muscular Tissue
Practice Questions
Nervous Tissue
Practice Questions
Cardiovascular System Histology
Practice Questions
Lymphoid Organs and Immune System
Practice Questions
Endocrine System Histology
Practice Questions
Respiratory System Histology
Practice Questions
Digestive System Histology
Practice Questions
Urinary and Reproductive System Histology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app