
Histology — MCQs

On this page
In stratified squamous epithelium, what is the shape of the cells in the basal layer?
Which glial cell type is primarily responsible for phagocytosis in the central nervous system?
Which of the following is the chief mineral of bone?
What type of epithelium lines the common bile duct?
All of the following are true about type-II pneumocytes, EXCEPT:
Elastic cartilage is found in which of the following locations?
Which of the following is true for tracheobronchial luminal neuroendocrine cells?
Myelin is stained by which of the following techniques?
Which of the following statements about Brunner's glands is FALSE?
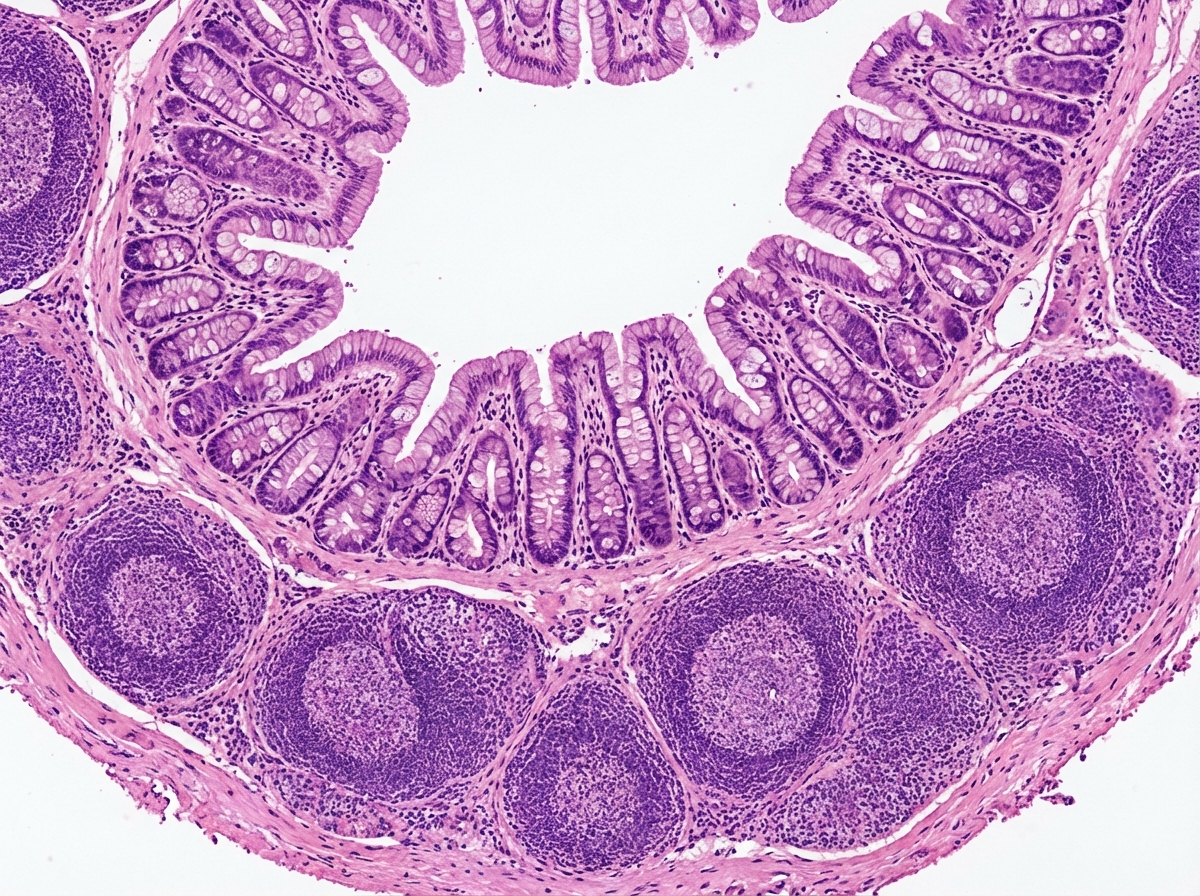
The given histological specimen is:
Practice by Chapter
Basic Tissue Types
Practice Questions
Cell Biology and Organelles
Practice Questions
Epithelial Tissue
Practice Questions
Connective Tissue
Practice Questions
Muscular Tissue
Practice Questions
Nervous Tissue
Practice Questions
Cardiovascular System Histology
Practice Questions
Lymphoid Organs and Immune System
Practice Questions
Endocrine System Histology
Practice Questions
Respiratory System Histology
Practice Questions
Digestive System Histology
Practice Questions
Urinary and Reproductive System Histology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app