
Histology — MCQs

On this page
Which of the following cells is the germ cell closest to the basal lamina in the seminiferous tubule?
Thyroid follicles are lined by which type of epithelium?
Stratum germinativum is synonymous to which layer of the epidermis?
For the growth of bone, which term is most appropriate?
The node of Ranvier is seen in which part of a neuron?
The ovary consists of all the following structures except:
Which is the strongest layer of the esophagus?
Ocular basement membrane is stained by which of the following?
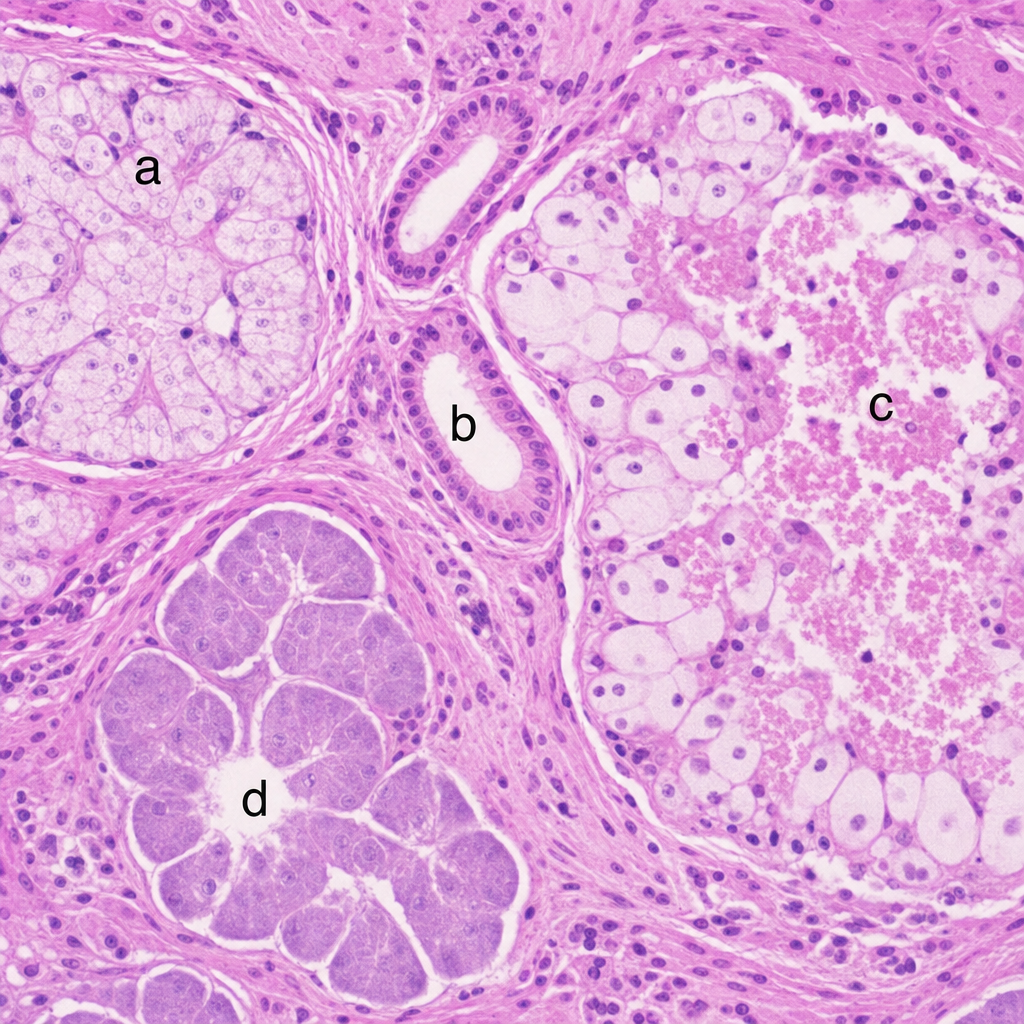
Which of the following cells are holocrine cells in the given slide?
What is true about the fallopian tube?
Practice by Chapter
Basic Tissue Types
Practice Questions
Cell Biology and Organelles
Practice Questions
Epithelial Tissue
Practice Questions
Connective Tissue
Practice Questions
Muscular Tissue
Practice Questions
Nervous Tissue
Practice Questions
Cardiovascular System Histology
Practice Questions
Lymphoid Organs and Immune System
Practice Questions
Endocrine System Histology
Practice Questions
Respiratory System Histology
Practice Questions
Digestive System Histology
Practice Questions
Urinary and Reproductive System Histology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app