
Histology — MCQs

On this page
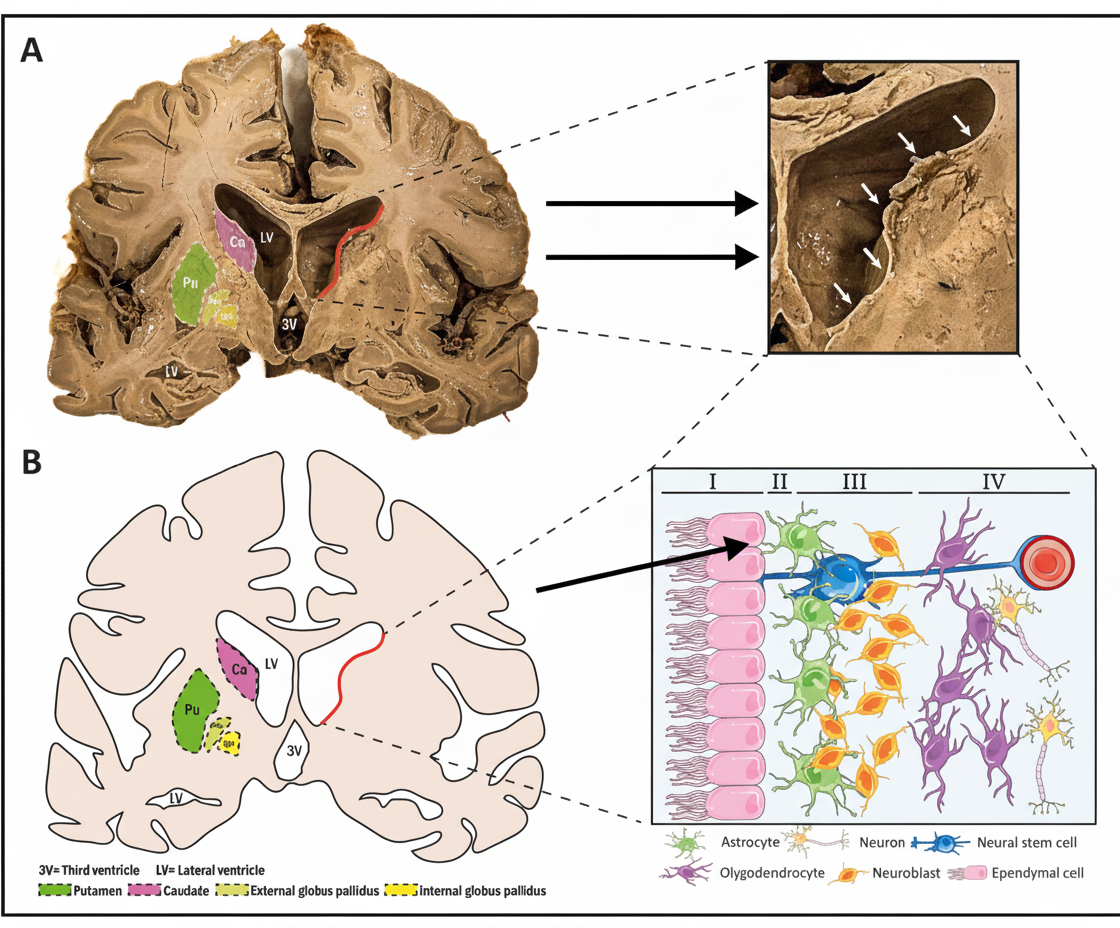
What is the type of epithelium lining the structures indicated by arrows in the provided diagram of the brain?
Which region of the lymph node is T cell dependent?
Which band in a sarcomere does not overlap with actin?
What is the specific name for tissue macrophages?
Type of collagen present in circumvallate sutures?
What filament is present in the H zone of a sarcomere?
What describes the anal transition zone?
Which of the following layers of the GIT is absent in the esophagus?
Where are Meissner's plexuses located?
Which of the following is NOT a feature of neuroglia cells?
Practice by Chapter
Basic Tissue Types
Practice Questions
Cell Biology and Organelles
Practice Questions
Epithelial Tissue
Practice Questions
Connective Tissue
Practice Questions
Muscular Tissue
Practice Questions
Nervous Tissue
Practice Questions
Cardiovascular System Histology
Practice Questions
Lymphoid Organs and Immune System
Practice Questions
Endocrine System Histology
Practice Questions
Respiratory System Histology
Practice Questions
Digestive System Histology
Practice Questions
Urinary and Reproductive System Histology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app