
Histology — MCQs

On this page
The portal acinus in the liver is centered on?
Goblet cells are not seen in which of the following locations?
Which of the following systems does NOT contain neuro-epithelium type of sensory receptors?
Urothelium is absent in which of the following structures?
Auerbach's plexus is present in which part of the gastrointestinal tract?
What type of epithelium lines the maxillary sinus?
Which of the following statements about the esophagus is FALSE?
The Pauter area of the spleen is formed by which of the following?
Which of the following is NOT a component of the juxtaglomerular apparatus?
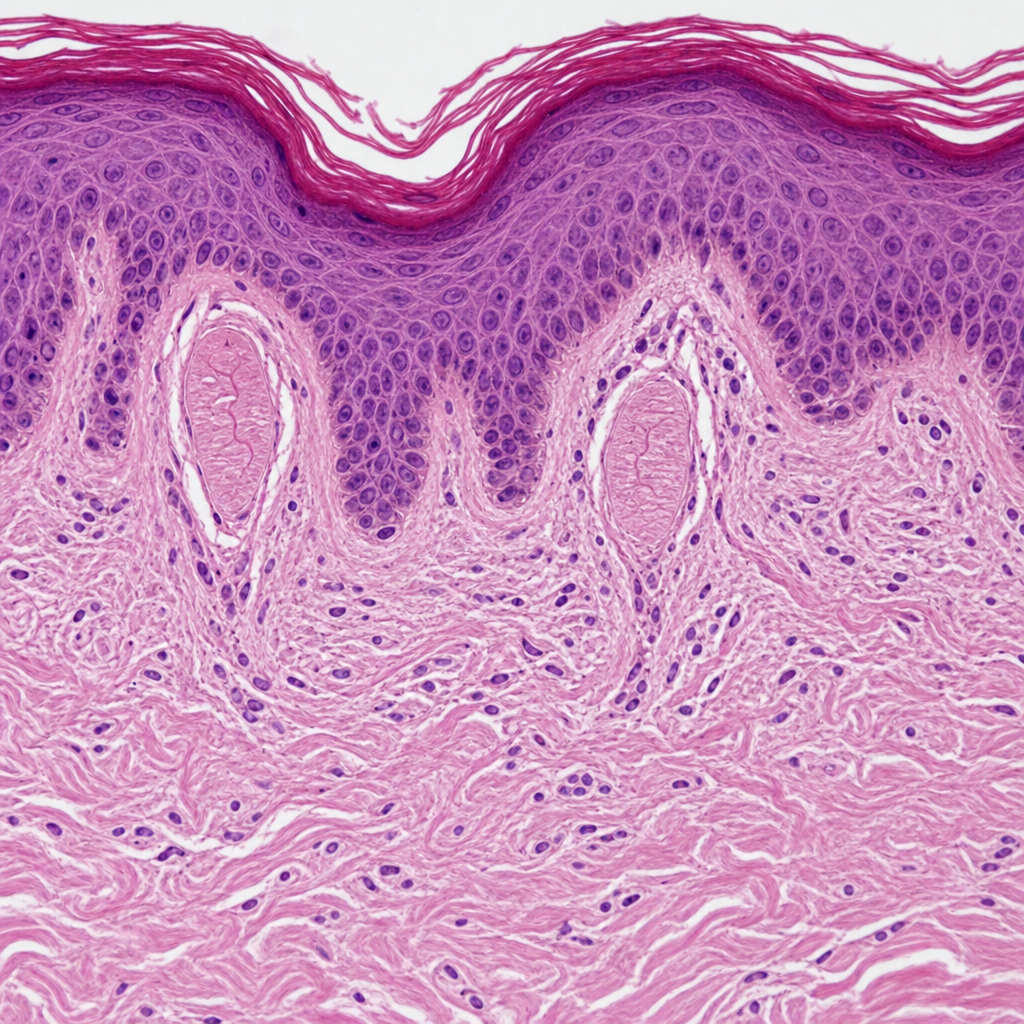
Which receptor is seen in this region?
Practice by Chapter
Basic Tissue Types
Practice Questions
Cell Biology and Organelles
Practice Questions
Epithelial Tissue
Practice Questions
Connective Tissue
Practice Questions
Muscular Tissue
Practice Questions
Nervous Tissue
Practice Questions
Cardiovascular System Histology
Practice Questions
Lymphoid Organs and Immune System
Practice Questions
Endocrine System Histology
Practice Questions
Respiratory System Histology
Practice Questions
Digestive System Histology
Practice Questions
Urinary and Reproductive System Histology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app