
Histology — MCQs

On this page
Which of the following is true about the apocrine gland?
The type of epithelium associated with the vermilion zone of the lips is:
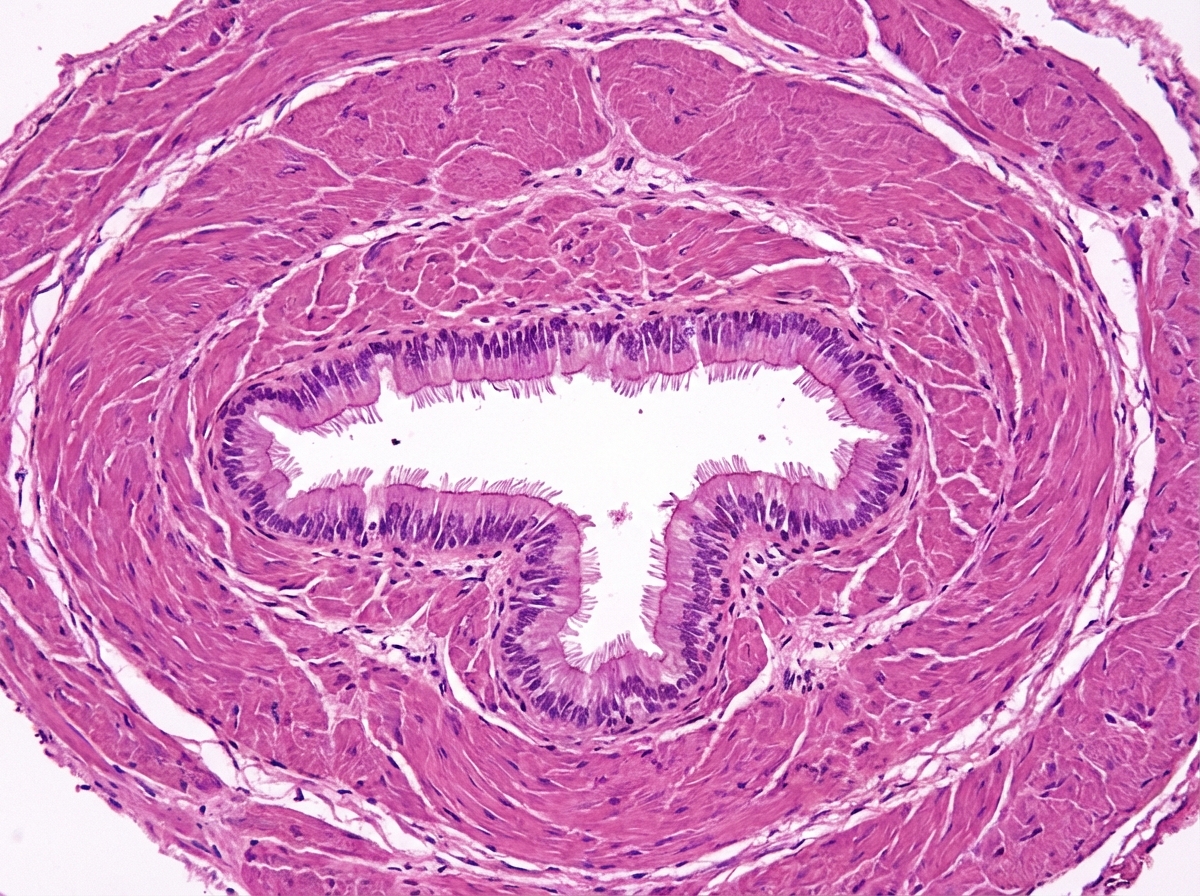
The following histological sample belongs to which of the following tissues?
Parietal peritoneum is lined by which type of epithelium?
Damage to nervous tissue is repaired by which of the following cell types?
Which type of collagen is present in the basement membrane?
Which stain is used for fat cells?
Which of the following is an example of facultative heterochromatin?
What is the most abundant type of collagen in hyaline cartilage?
Small intestine and colon are lined by which type of epithelium?
Practice by Chapter
Basic Tissue Types
Practice Questions
Cell Biology and Organelles
Practice Questions
Epithelial Tissue
Practice Questions
Connective Tissue
Practice Questions
Muscular Tissue
Practice Questions
Nervous Tissue
Practice Questions
Cardiovascular System Histology
Practice Questions
Lymphoid Organs and Immune System
Practice Questions
Endocrine System Histology
Practice Questions
Respiratory System Histology
Practice Questions
Digestive System Histology
Practice Questions
Urinary and Reproductive System Histology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app