
Histology — MCQs

On this page
What are the supporting cells of the testes?
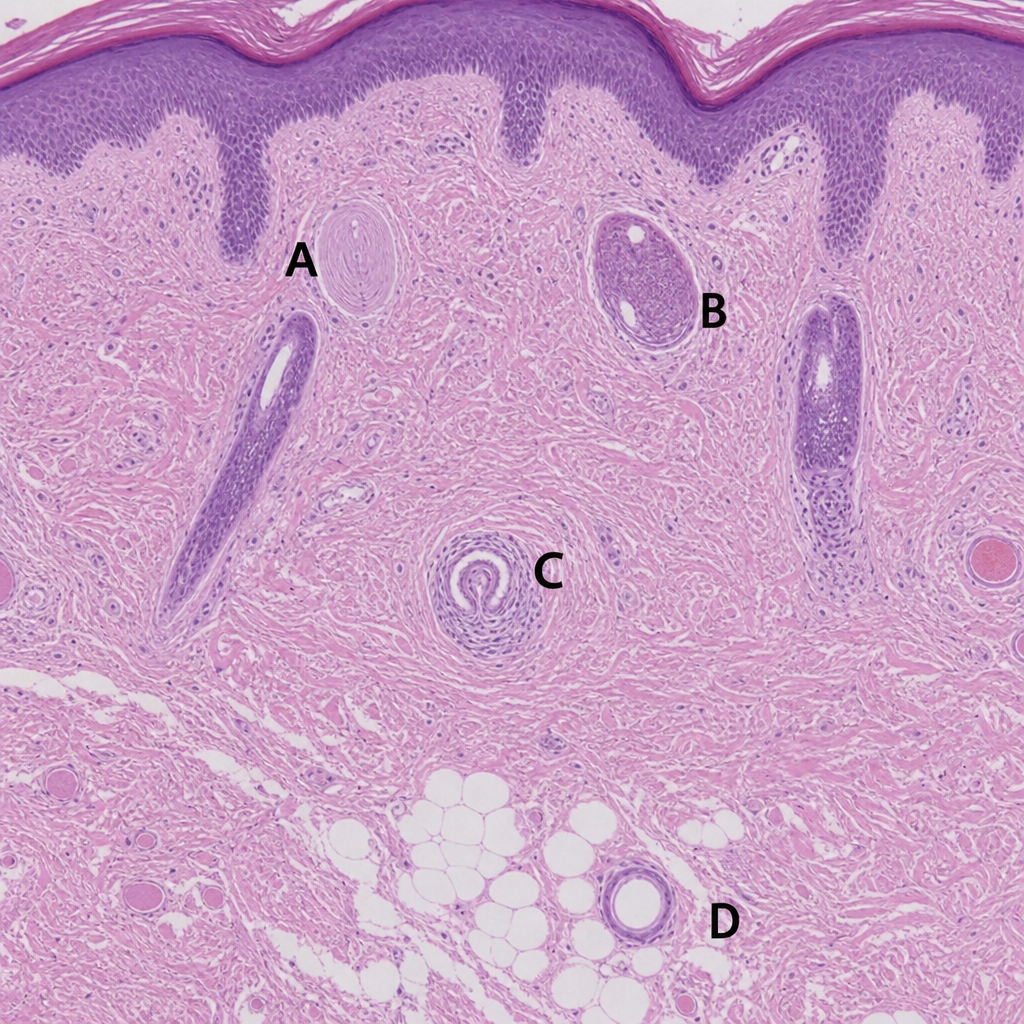
In the provided histology image, which lettered area represents the structure primarily involved in pain relief when activated by deep pressure and high-frequency vibration?
What does 'portal acinus' refer to?
Which of the following statements about elastic cartilage is true?
Which cells demonstrate a 1:1 ratio of myelination?
Which of the following junctions does not provide rigidity and support?
All of the following are components of the white pulp of the spleen, except?
What type of cartilage is present in the ear pinna?
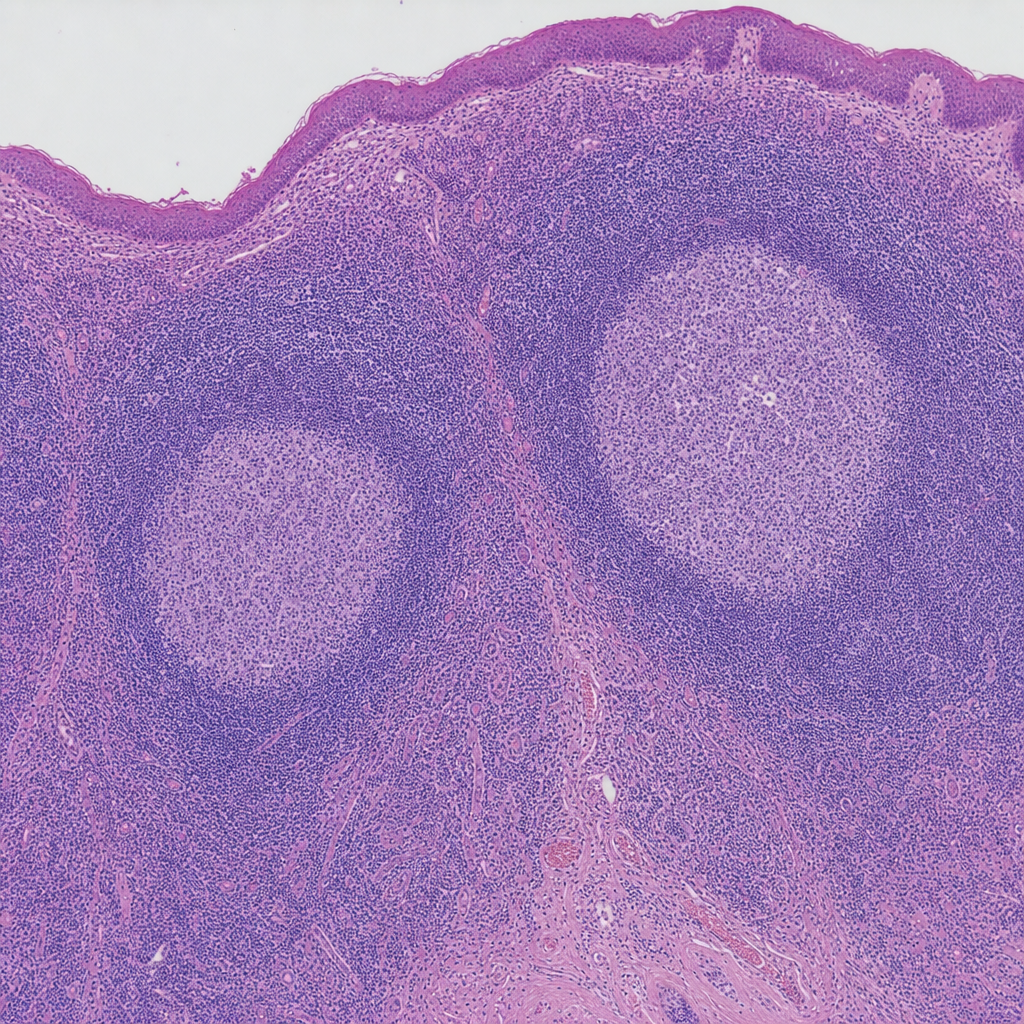
The following hematoxylin and eosin stained biopsy is from which tissue?
Protoplasmic astrocytes are located in which part of the central nervous system?
Practice by Chapter
Basic Tissue Types
Practice Questions
Cell Biology and Organelles
Practice Questions
Epithelial Tissue
Practice Questions
Connective Tissue
Practice Questions
Muscular Tissue
Practice Questions
Nervous Tissue
Practice Questions
Cardiovascular System Histology
Practice Questions
Lymphoid Organs and Immune System
Practice Questions
Endocrine System Histology
Practice Questions
Respiratory System Histology
Practice Questions
Digestive System Histology
Practice Questions
Urinary and Reproductive System Histology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app