
Histology — MCQs

On this page
Which of the following cells proliferate from the top to the bottom of villi?
Transitional epithelium is seen in which of the following structures?
In which type of glands are serous demilunes typically found?
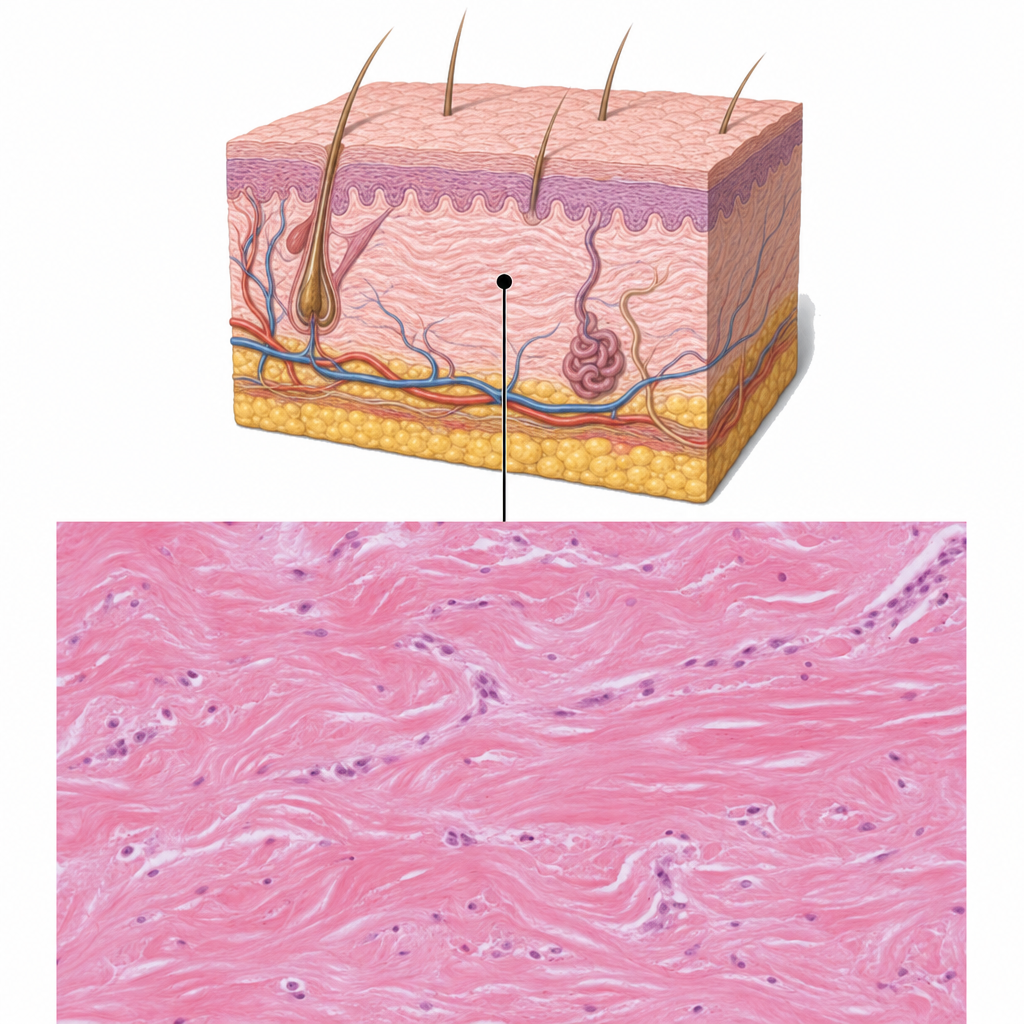
What type of connective tissue is present in the indicated area?
Paneth cells are mainly found in the bases of the crypts in the small intestine. All of the following are true about Paneth cells, EXCEPT:
Gomori's aldehyde fuchsin specifically stains which of the following?
Which of the following is the weakest type of cartilage?
All of the following are macrophages except:
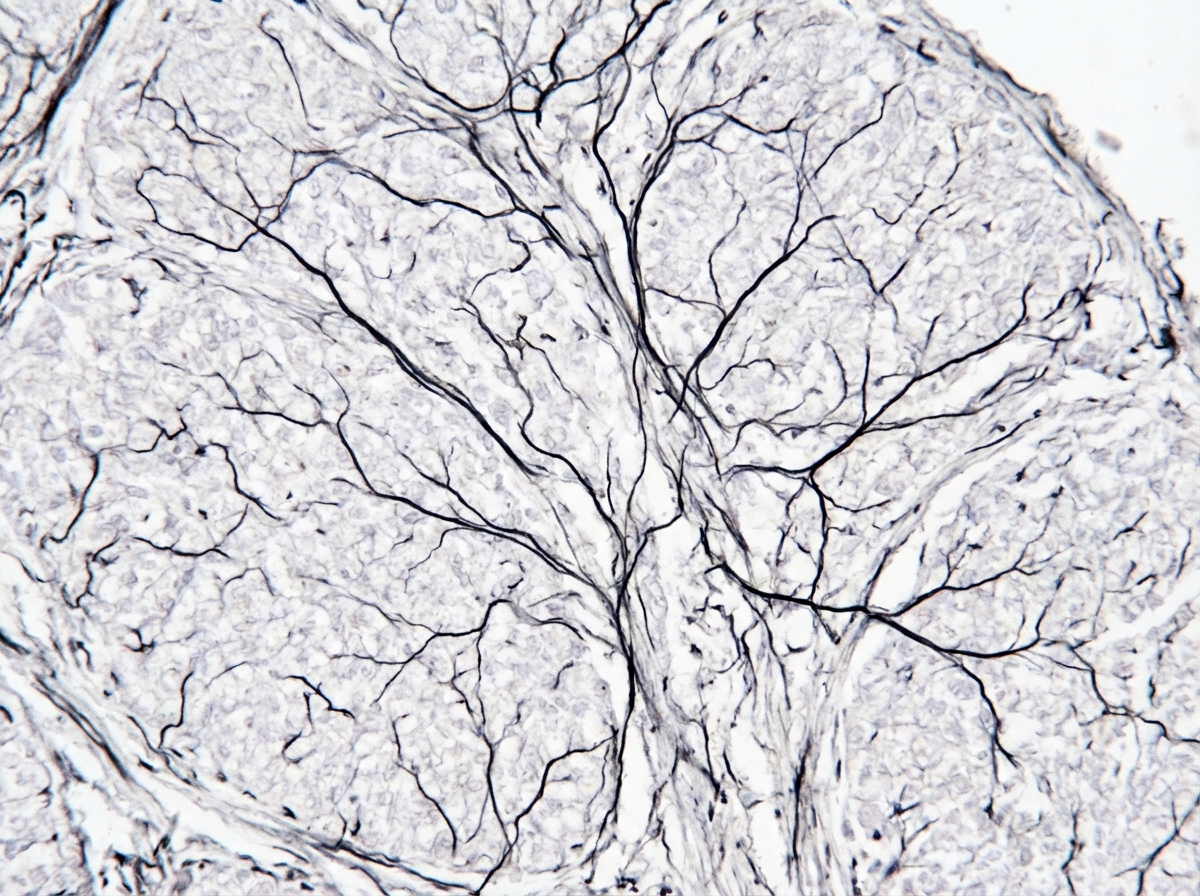
The type of collagen depicted in the staining is:
What structure is present between two successive z-lines?
Practice by Chapter
Basic Tissue Types
Practice Questions
Cell Biology and Organelles
Practice Questions
Epithelial Tissue
Practice Questions
Connective Tissue
Practice Questions
Muscular Tissue
Practice Questions
Nervous Tissue
Practice Questions
Cardiovascular System Histology
Practice Questions
Lymphoid Organs and Immune System
Practice Questions
Endocrine System Histology
Practice Questions
Respiratory System Histology
Practice Questions
Digestive System Histology
Practice Questions
Urinary and Reproductive System Histology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app