
Histology — MCQs

On this page
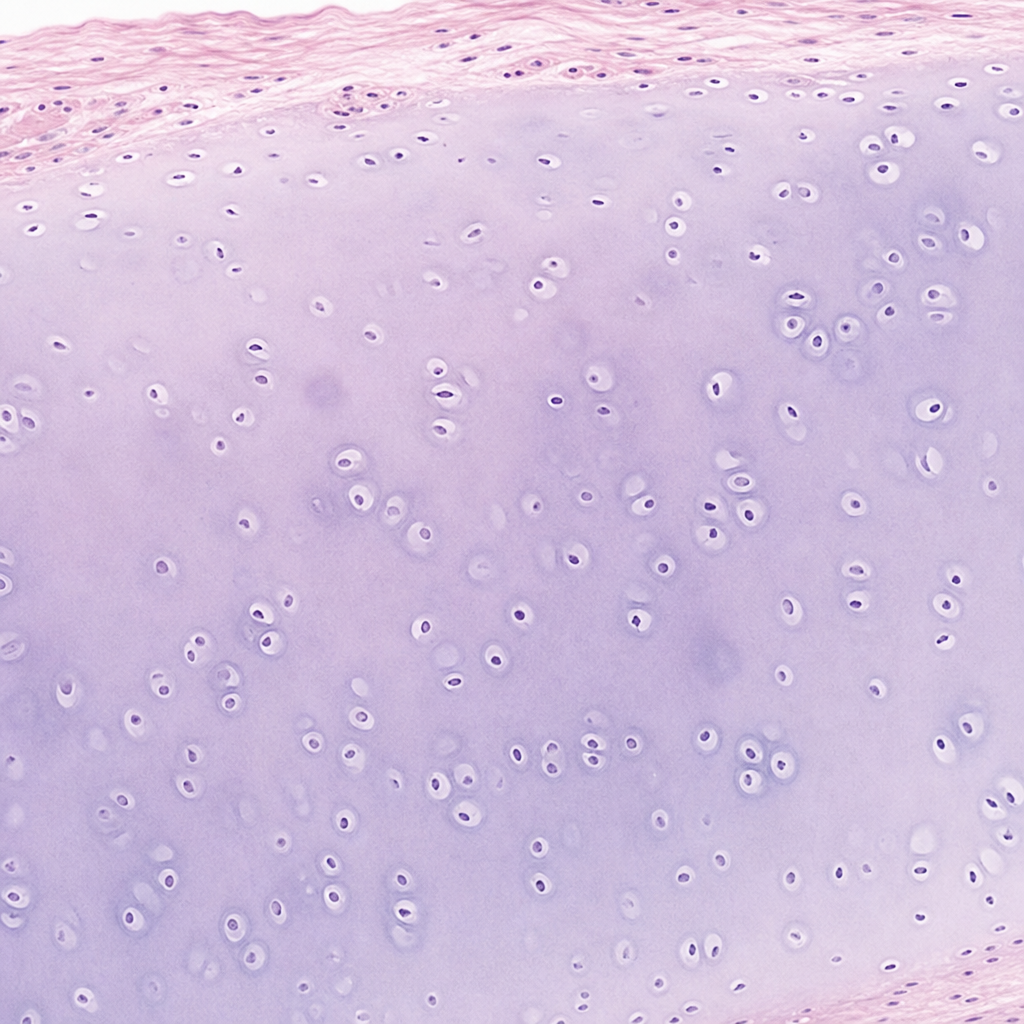
The type of cartilage shown in the color plate is:
Which of the following cells is NOT present in the parathyroid gland?
Fenestrated capillaries are present in which of the following locations?
Which of the following cellular structures is functionally equivalent to the rough endoplasmic reticulum?
Schwann cells are supporting cells of:
Lamin is present in:
Which of the following structures histologically shows Henle's and Huxley's layers?
Which stain is used to detect myelin?
Which of the following is true about articular cartilage?
Which of the following statements about osteoclasts is not true?
Practice by Chapter
Basic Tissue Types
Practice Questions
Cell Biology and Organelles
Practice Questions
Epithelial Tissue
Practice Questions
Connective Tissue
Practice Questions
Muscular Tissue
Practice Questions
Nervous Tissue
Practice Questions
Cardiovascular System Histology
Practice Questions
Lymphoid Organs and Immune System
Practice Questions
Endocrine System Histology
Practice Questions
Respiratory System Histology
Practice Questions
Digestive System Histology
Practice Questions
Urinary and Reproductive System Histology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app