
Functional Anatomy — MCQs

On this page
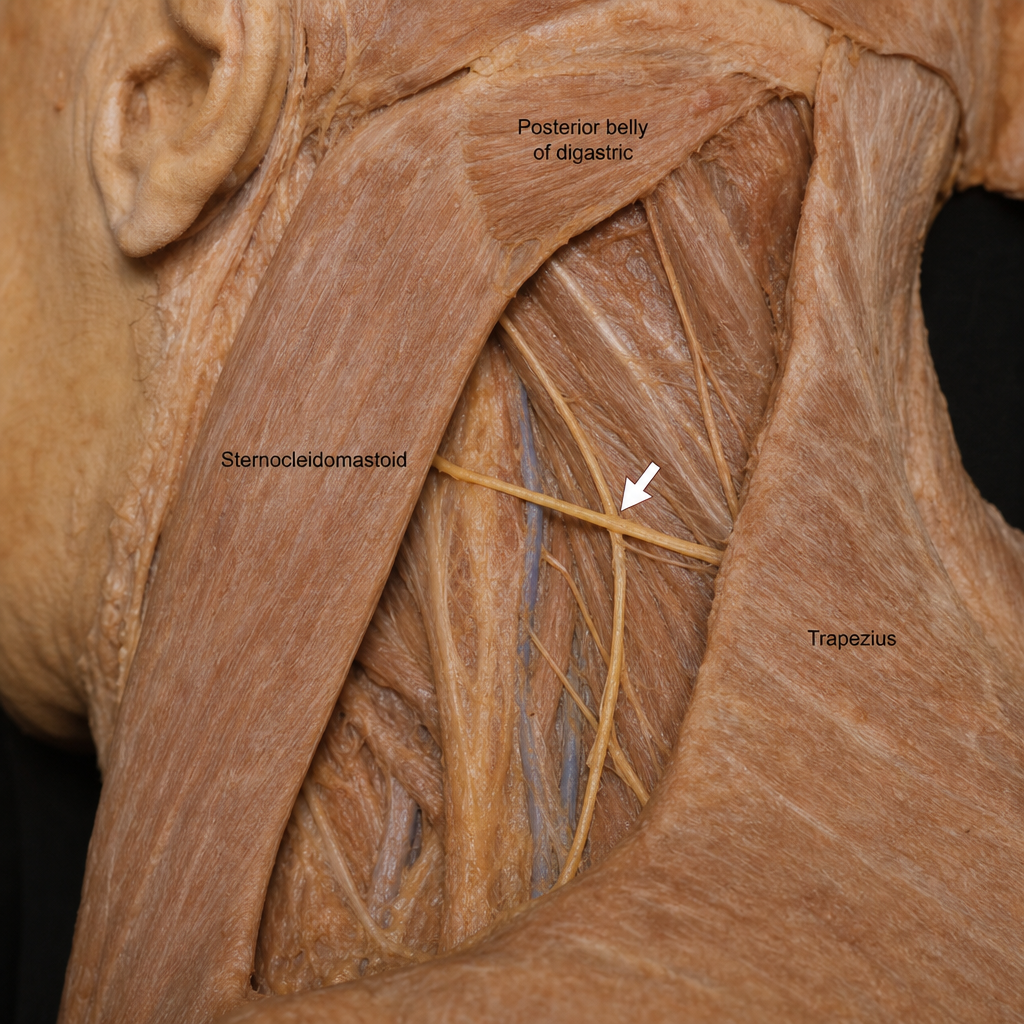
A 28-year-old woman undergoes excision of an enlarged lymph node in the posterior triangle of the neck. Two weeks post-operatively she is unable to shrug her left shoulder. Nerve conduction studies confirm injury to the arrowed nerve (Image 1) as well as a separate injury to the long thoracic nerve, accounting for a newly noted winged scapula on the ipsilateral side. Which of the following best explains why TWO distinct nerve injuries are required to account for both motor deficits observed in this patient?
Practice by Chapter
Anatomical Basis of Movement
Practice Questions
Biomechanics of Joints
Practice Questions
Functional Anatomy of Respiratory System
Practice Questions
Functional Anatomy of Cardiovascular System
Practice Questions
Functional Anatomy of Digestive System
Practice Questions
Functional Anatomy of Urinary System
Practice Questions
Functional Anatomy of Reproductive System
Practice Questions
Neuroanatomical Basis of Functions
Practice Questions
Functional Correlations in Clinical Practice
Practice Questions
Anatomical Aspects of Exercise Physiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app