
Embryology and Development — MCQs

On this page
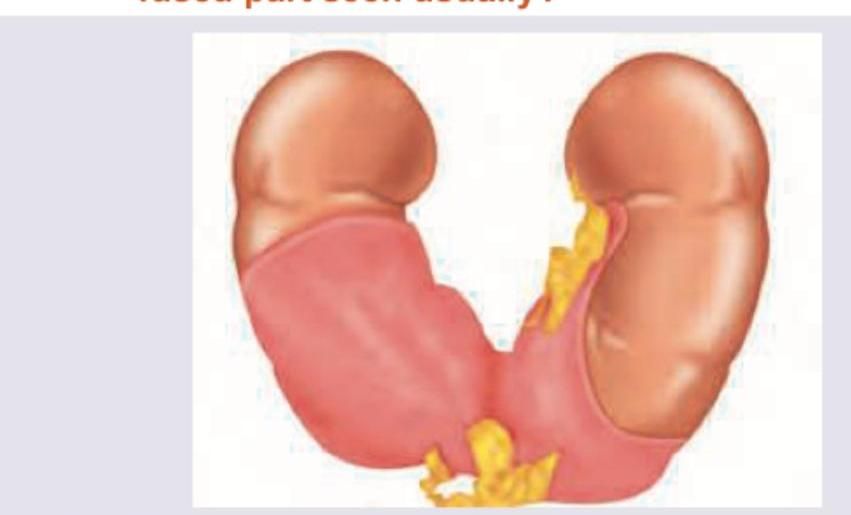
A 28 -year-old male was found to have a condition shown in the image below. At which level is the fused part seen usually?
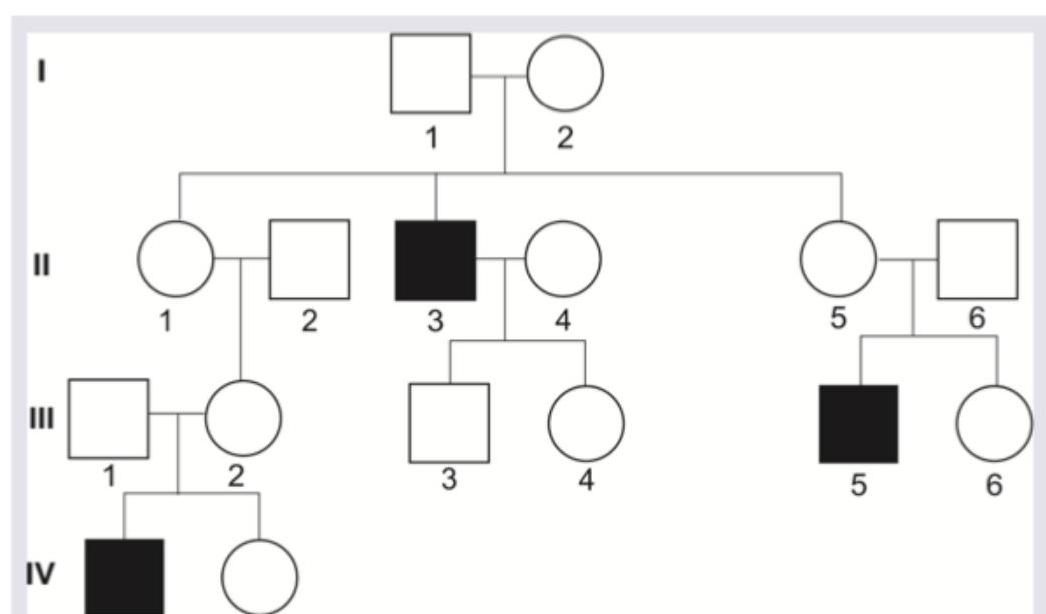
Identify the inheritance pattern shown below.
Which one of the following best describes craniosynostosis?
Which of the following statements with regard to Meckel's Diverticulum are correct? 1. It represents a persistent remnant of the vitellointestinal duct. 2. It is a true diverticulum of gastrointestinal tract. 3. It is most commonly found on anti-mesenteric border of ileum. 4. Heterotopic mucosa is present in 50-60% of patients. Select the correct answer using the code given below:
A meningomyelocele is most commonly situated in the
Monoamniotic monochorionic twins develop when the division of cell mass occurs
The lungs are derived from an out-pouching of the primitive foregut during which period of intrauterine life?
Regarding “conjoined twins”, which of the following statements is/are true? 1. These are always monozygotic 2. These result when division occurs before the embryonic disc is formed 3. Most common variety is thoracopagus Select the correct answer using the code given below:
The umbilical cord normally contains:
The external opening of branchial fistula is present in :
Practice by Chapter
Gametogenesis and Fertilization
Practice Questions
Early Embryonic Development
Practice Questions
Placentation
Practice Questions
Development of Nervous System
Practice Questions
Development of Cardiovascular System
Practice Questions
Development of Gastrointestinal System
Practice Questions
Development of Urogenital System
Practice Questions
Development of Musculoskeletal System
Practice Questions
Development of Head and Neck
Practice Questions
Congenital Anomalies
Practice Questions
Teratology
Practice Questions
Molecular Mechanisms in Development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app