
Embryology and Development — MCQs

On this page
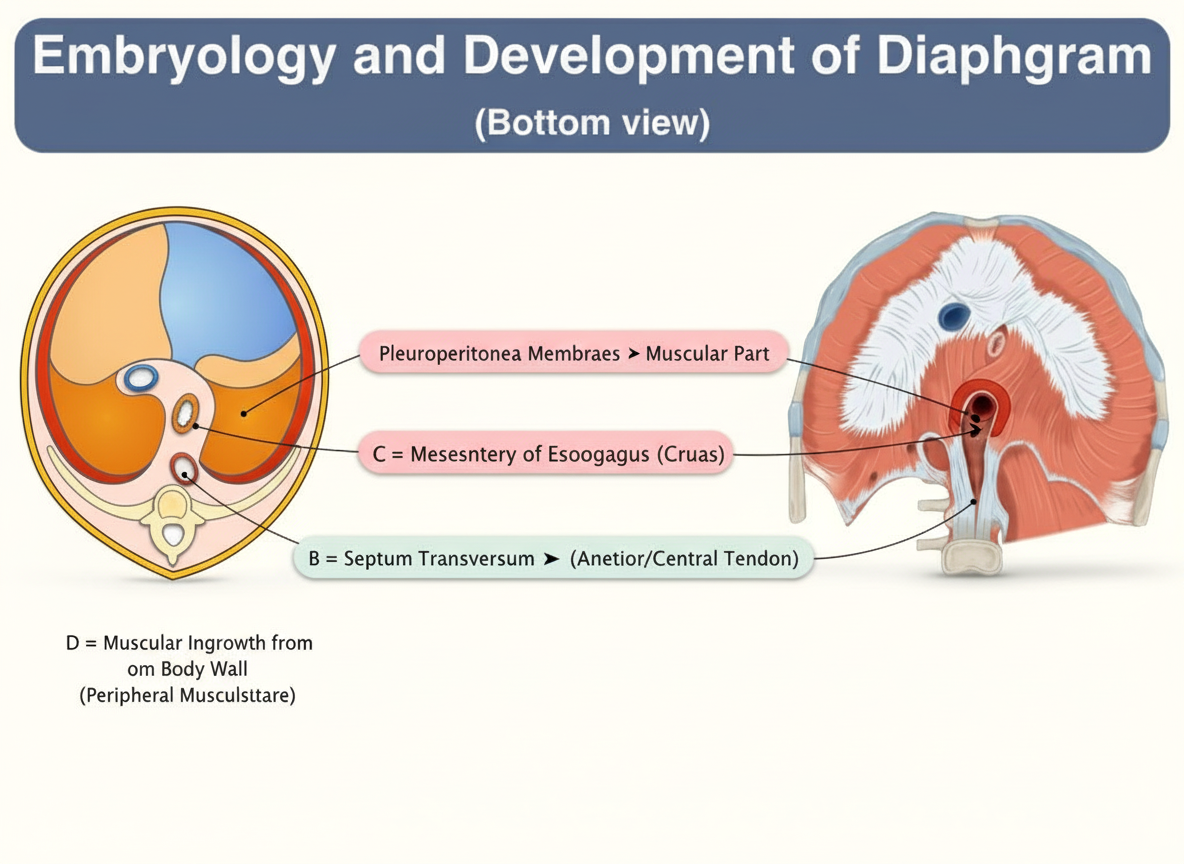
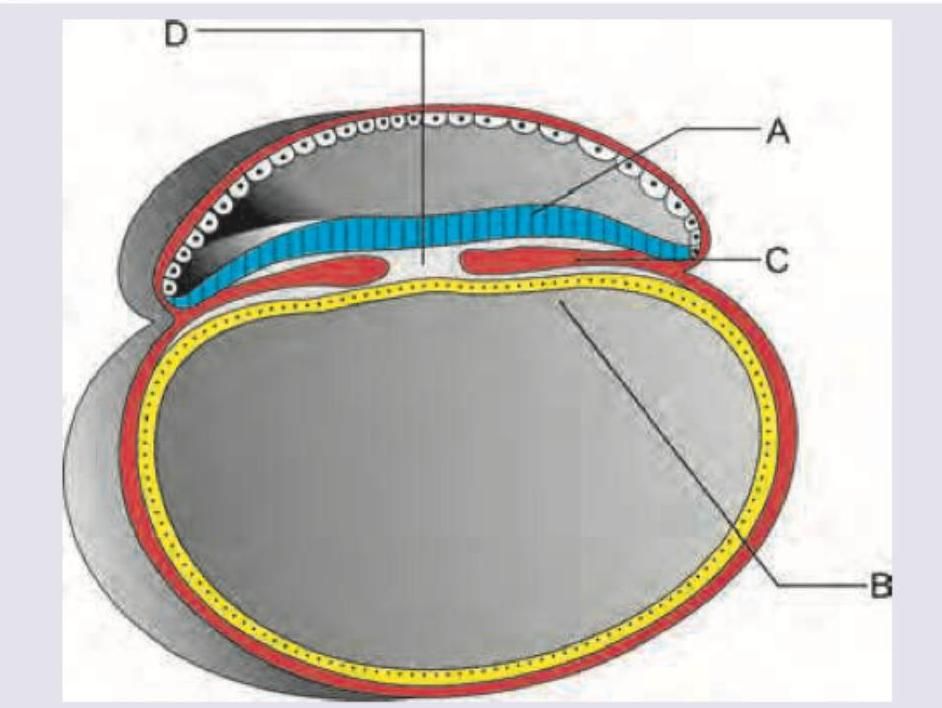
The diagram given below depicts the various parts from which the diaphragm develops. Defect in which part most commonly leads to congenital diaphragmatic hernia? (AIIMS May 2016)
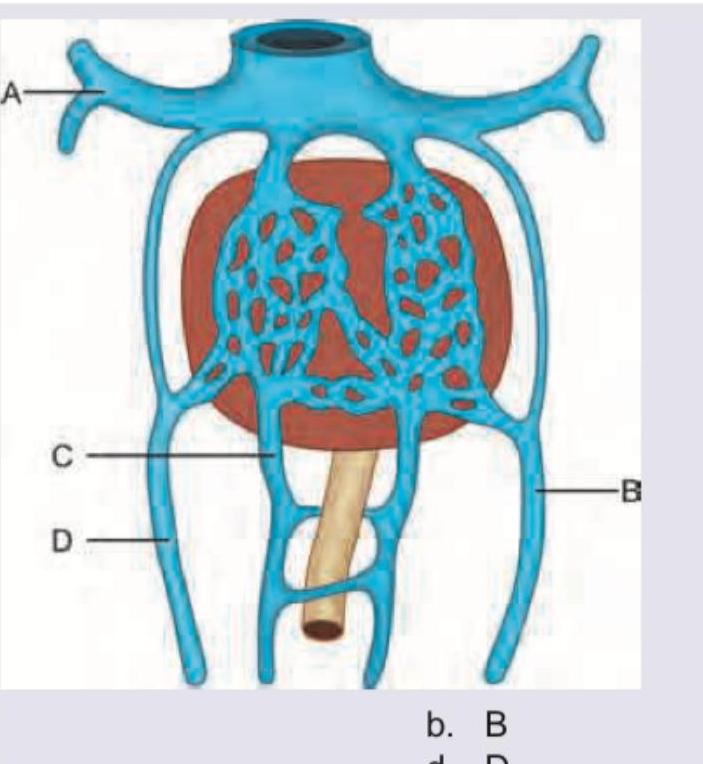
Portal vein develops from which of these structures? (AIIMS May 2016)
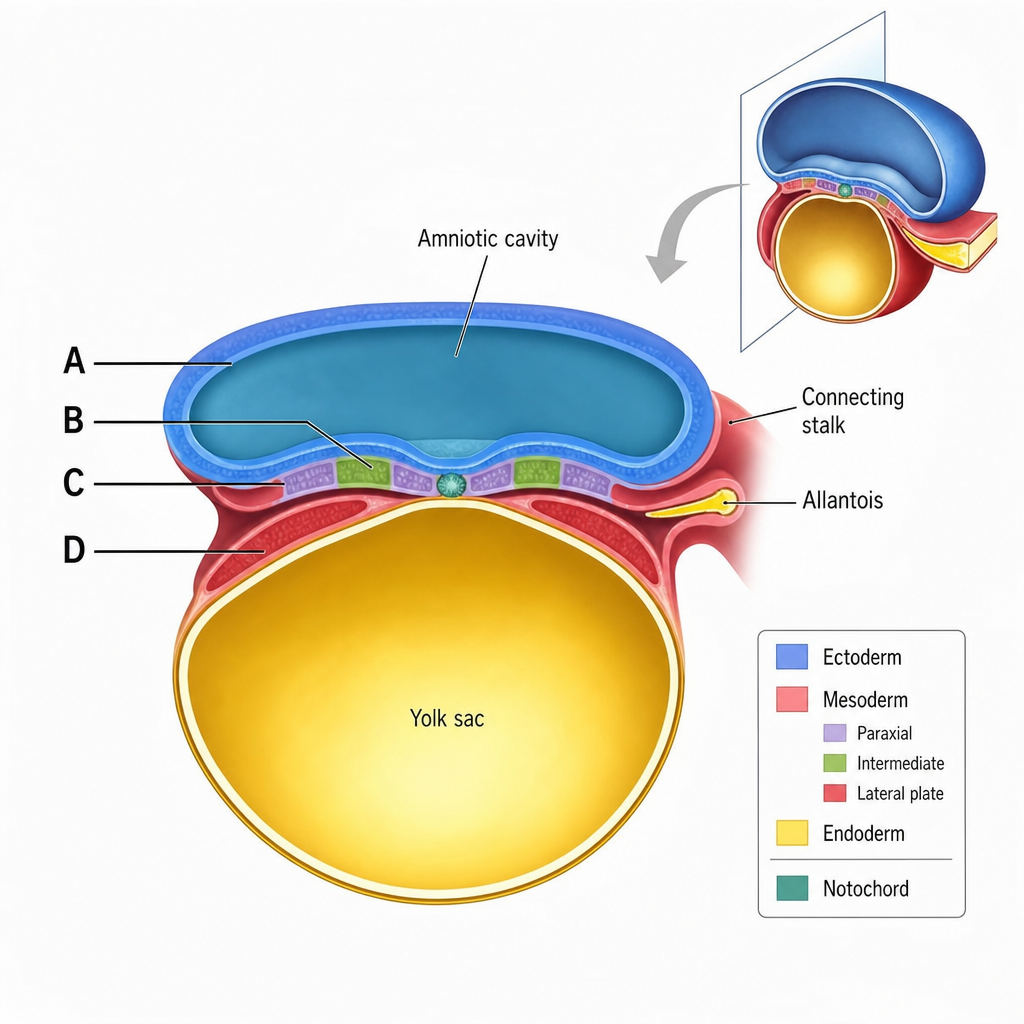
Which of the following marked structures would give rise to the heart?
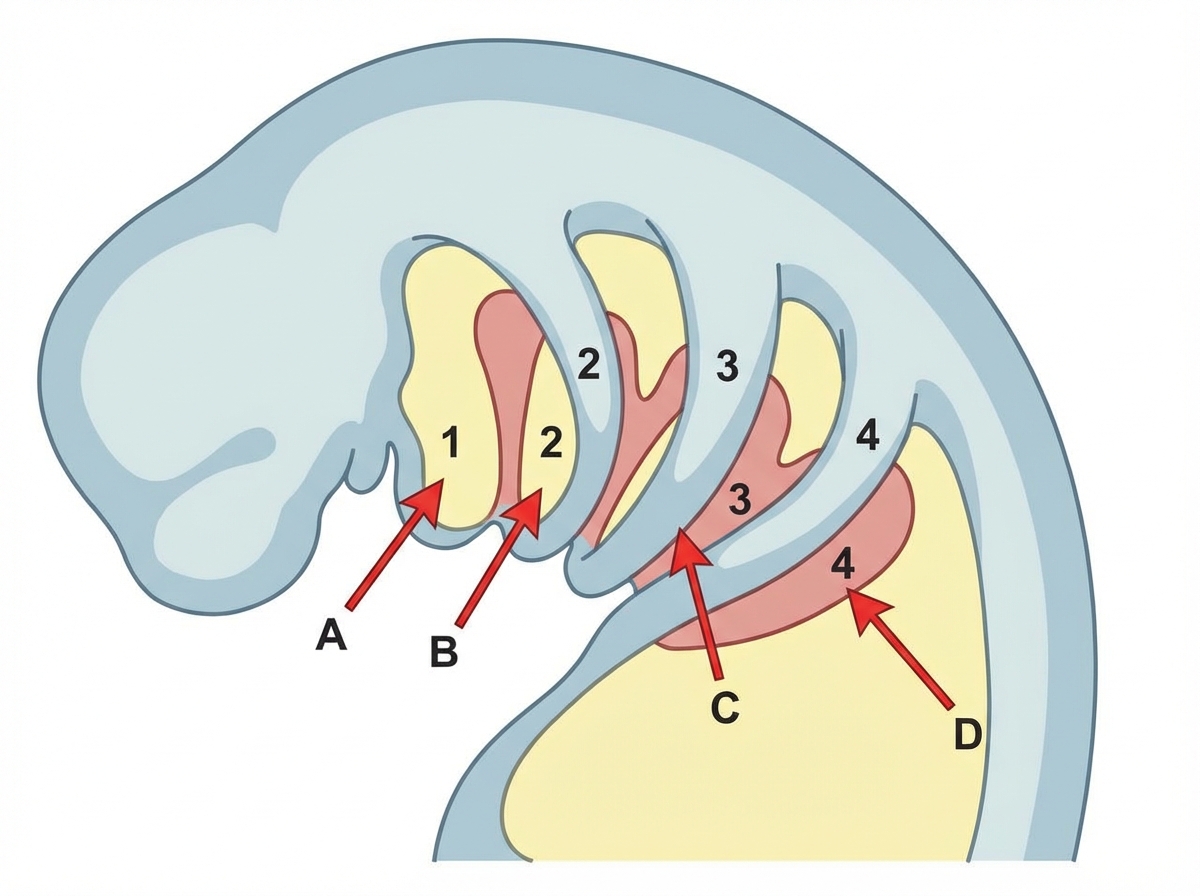
A young patient with absent thymus presents with tetany and hypoparathyroidism. Which of the following is a marked area in the picture defective in this condition?
Nucleus pulposus develops from: (AIIMS May 2018)
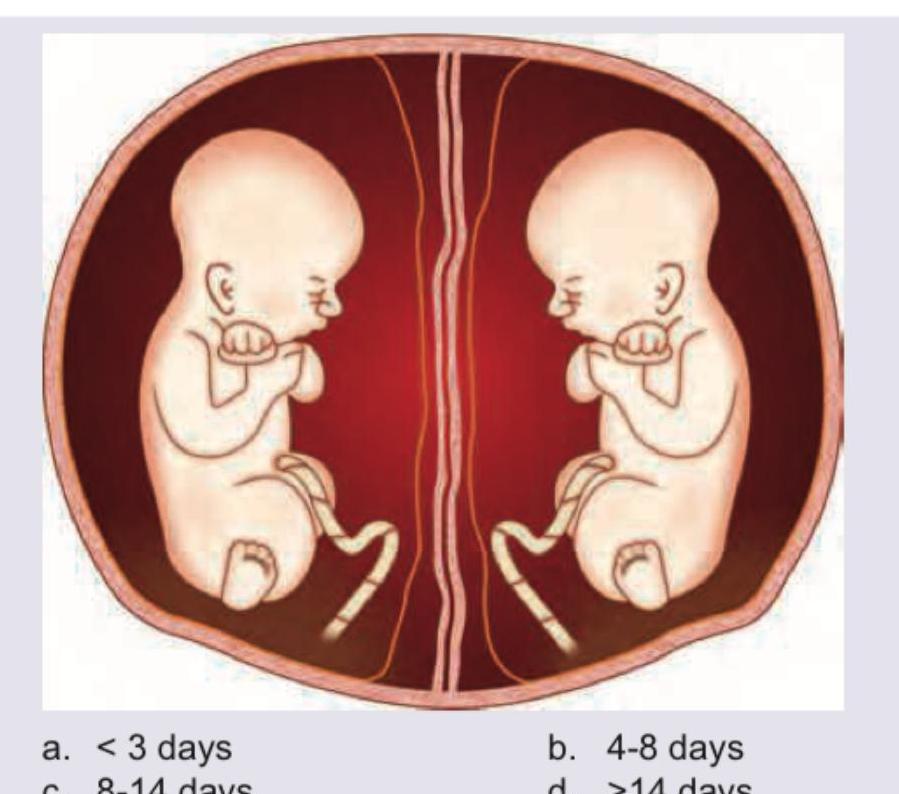
For the formation of the shown monozygotic twins, division should take place by
Which neural tube defect is shown here:
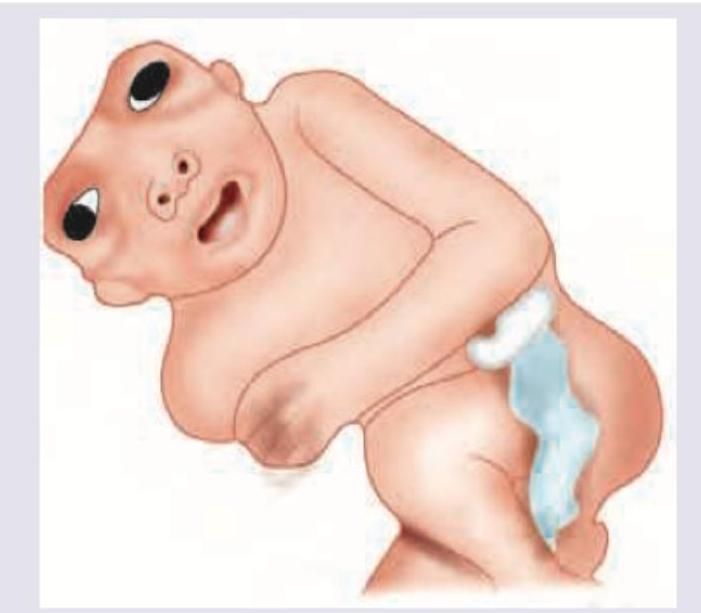
Name the neural tube defect shown here:
The image shows:
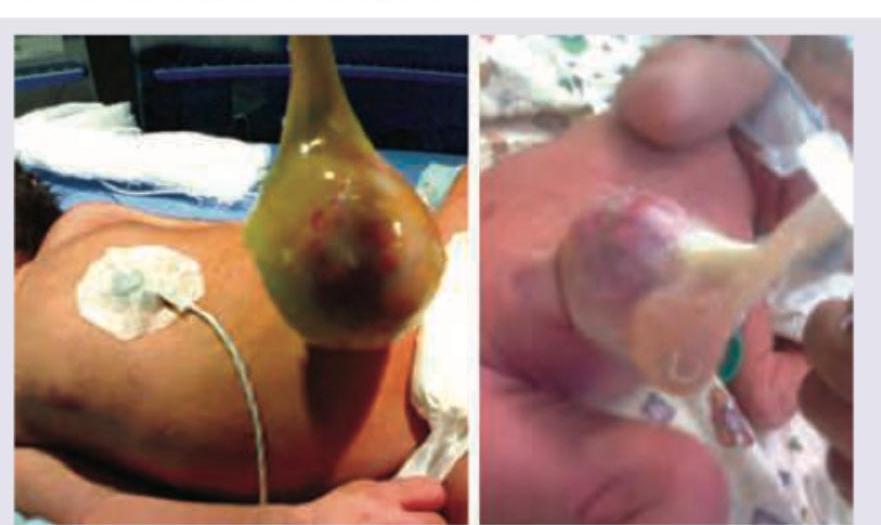
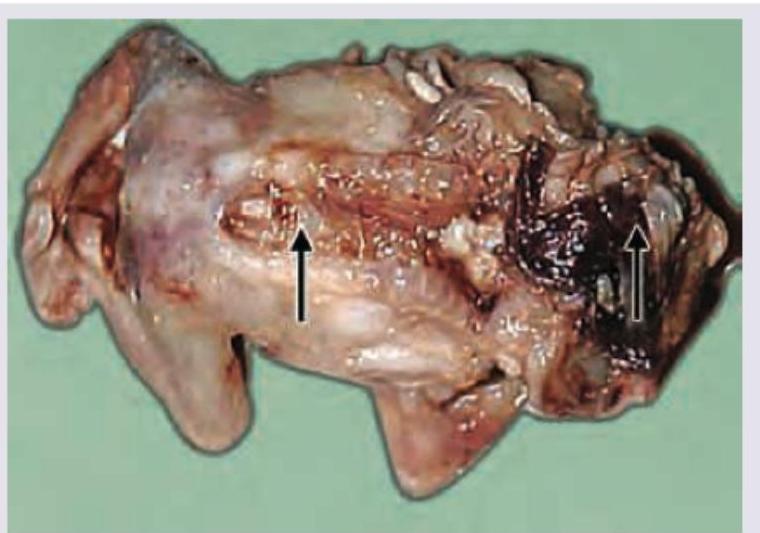
A newborn presents with a mass in the sacrococcygeal region as shown in the image. Identify the condition:

Practice by Chapter
Gametogenesis and Fertilization
Practice Questions
Early Embryonic Development
Practice Questions
Placentation
Practice Questions
Development of Nervous System
Practice Questions
Development of Cardiovascular System
Practice Questions
Development of Gastrointestinal System
Practice Questions
Development of Urogenital System
Practice Questions
Development of Musculoskeletal System
Practice Questions
Development of Head and Neck
Practice Questions
Congenital Anomalies
Practice Questions
Teratology
Practice Questions
Molecular Mechanisms in Development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app