
Embryology and Development — MCQs

On this page
Destruction of ovaries prior to the 7th week following fertilization results in what?
Metanephros develops during which week of embryonic development?
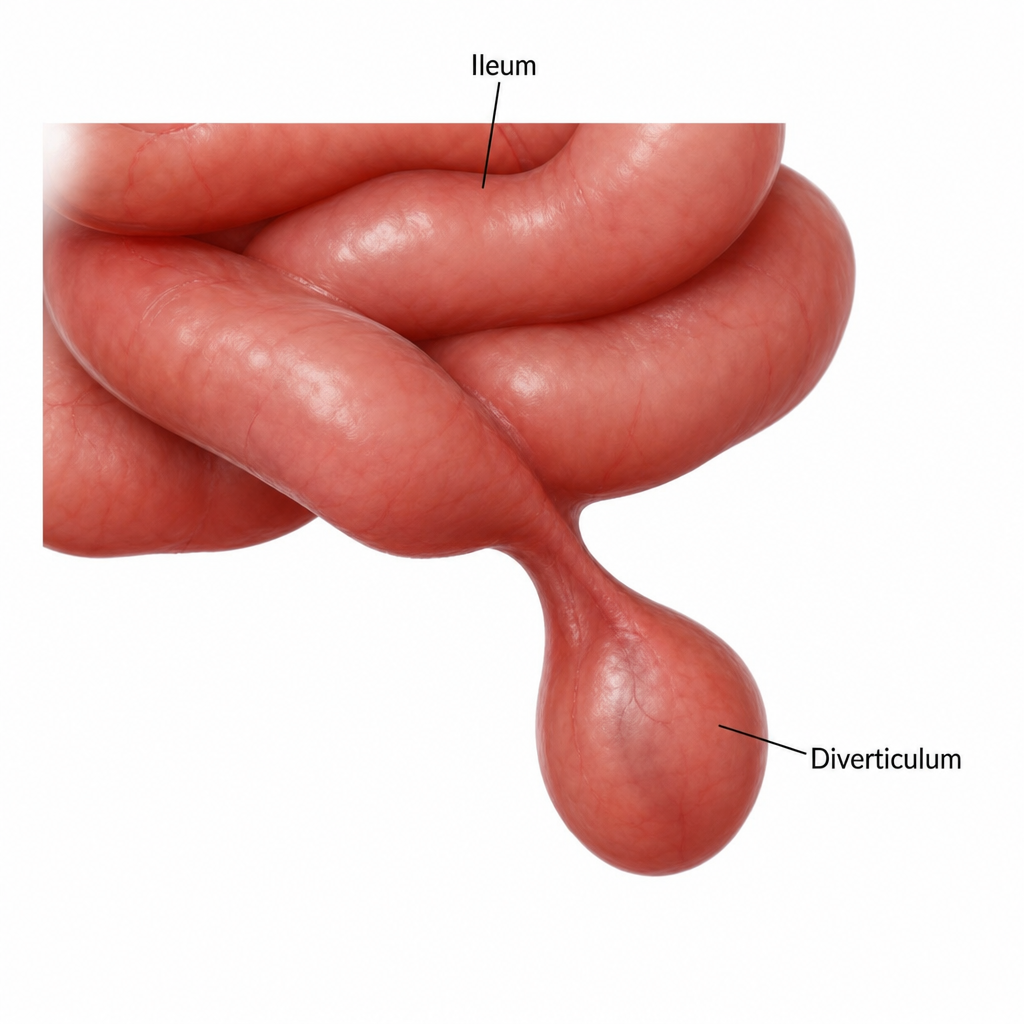
The congenital abnormality of the ileum illustrated below is related to persistence of which of the following structures?
A male neonate develops small-bowel obstruction due to malrotation of the midgut segment. An x-ray of the abdomen confirms the presence of small-bowel obstruction. The neonate undergoes an emergency laparotomy, untwisting of the malrotated intestines, and partial small-bowel resection for intestinal infarction. Which of the following statements is true of the small intestine (jejunum and ileum)?
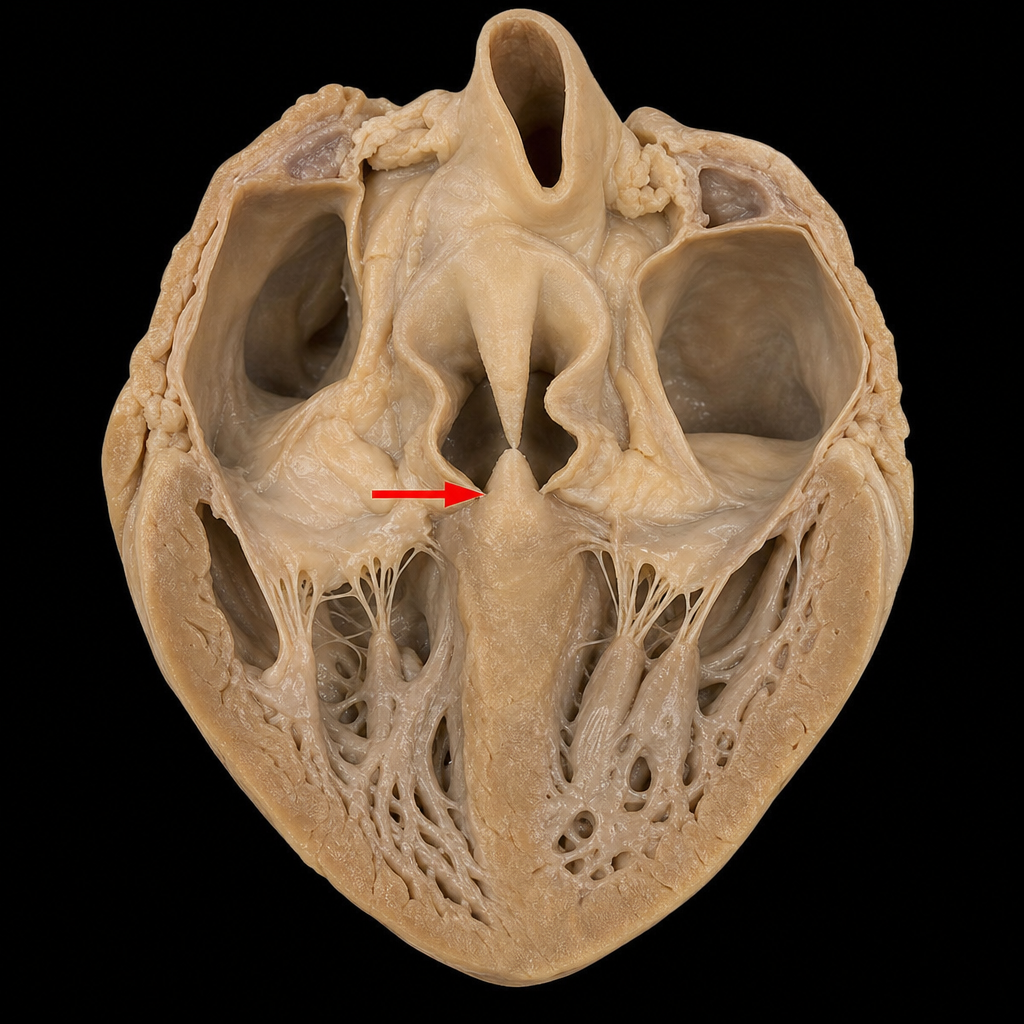
The membranous part of the interventricular septum (marked with a red arrow) is derived from which of the following?
Neural tube formation occurs when?
The primitive uteroplacental circulation is functionally established during which period of embryonic/fetal development?
Endochondral ossification is seen in:
The collecting ducts of the kidney develop from which embryonic structure?
A partial development of the aortopulmonary septum will result in which of the following?
Practice by Chapter
Gametogenesis and Fertilization
Practice Questions
Early Embryonic Development
Practice Questions
Placentation
Practice Questions
Development of Nervous System
Practice Questions
Development of Cardiovascular System
Practice Questions
Development of Gastrointestinal System
Practice Questions
Development of Urogenital System
Practice Questions
Development of Musculoskeletal System
Practice Questions
Development of Head and Neck
Practice Questions
Congenital Anomalies
Practice Questions
Teratology
Practice Questions
Molecular Mechanisms in Development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app