
Embryology and Development — MCQs

On this page
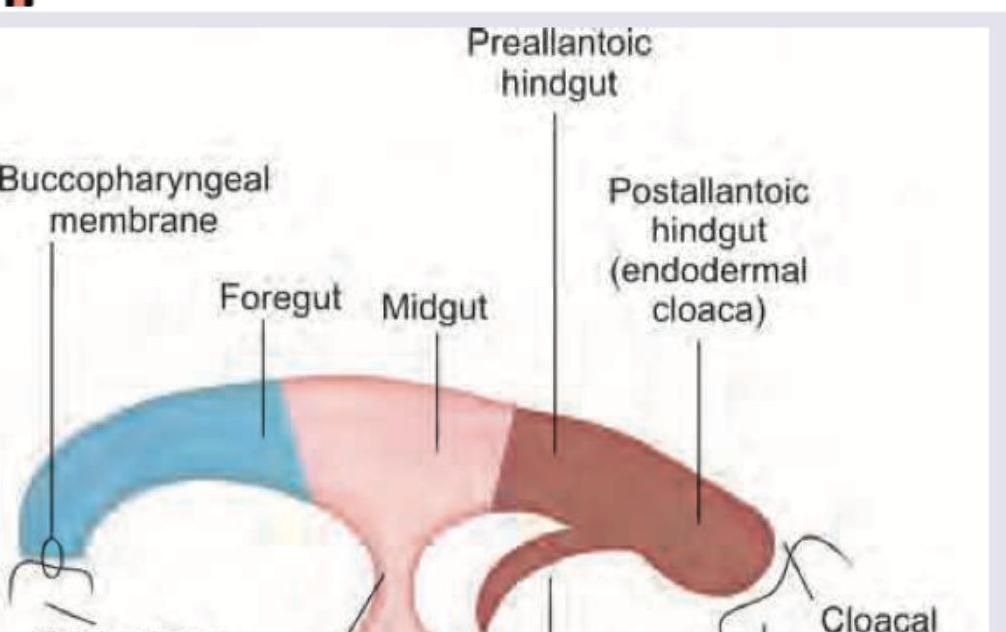
Which is correct sequence about the blood supply of the primitive gut?
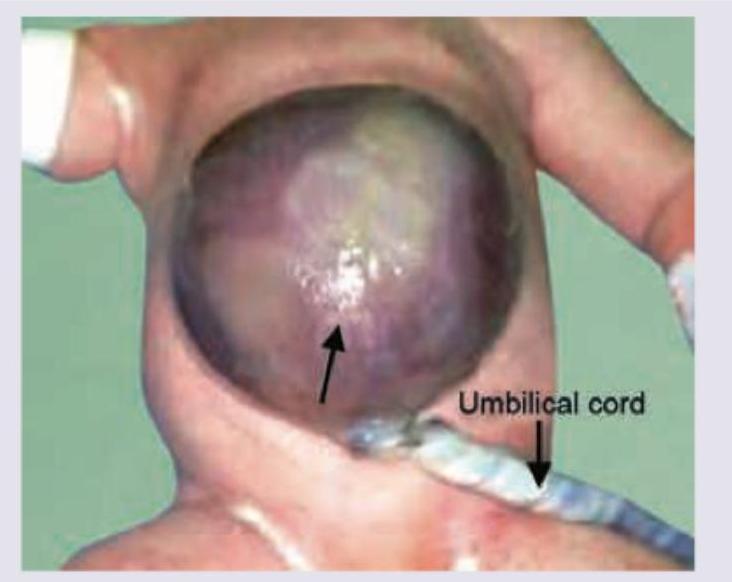
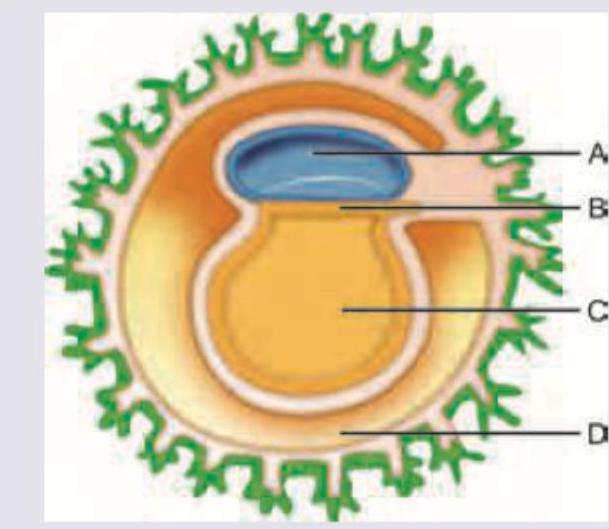
Which is wrong about the image given below?
The condition shown below is due to ?
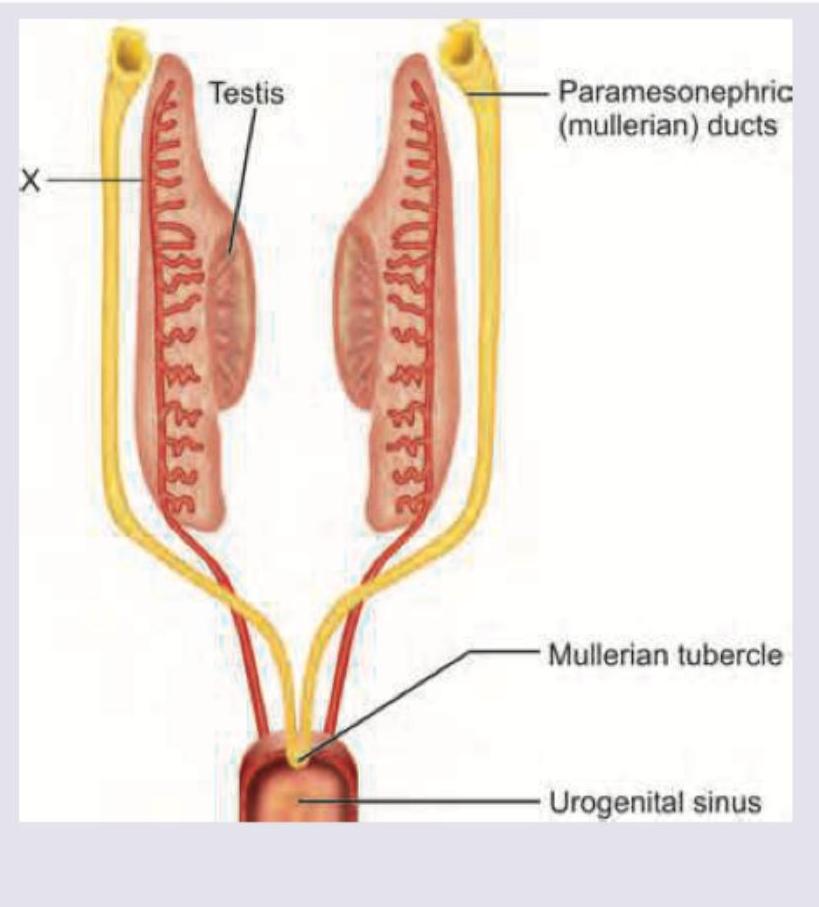
All of the following structures develop from the structure marked as $X$ in a male fetus except:
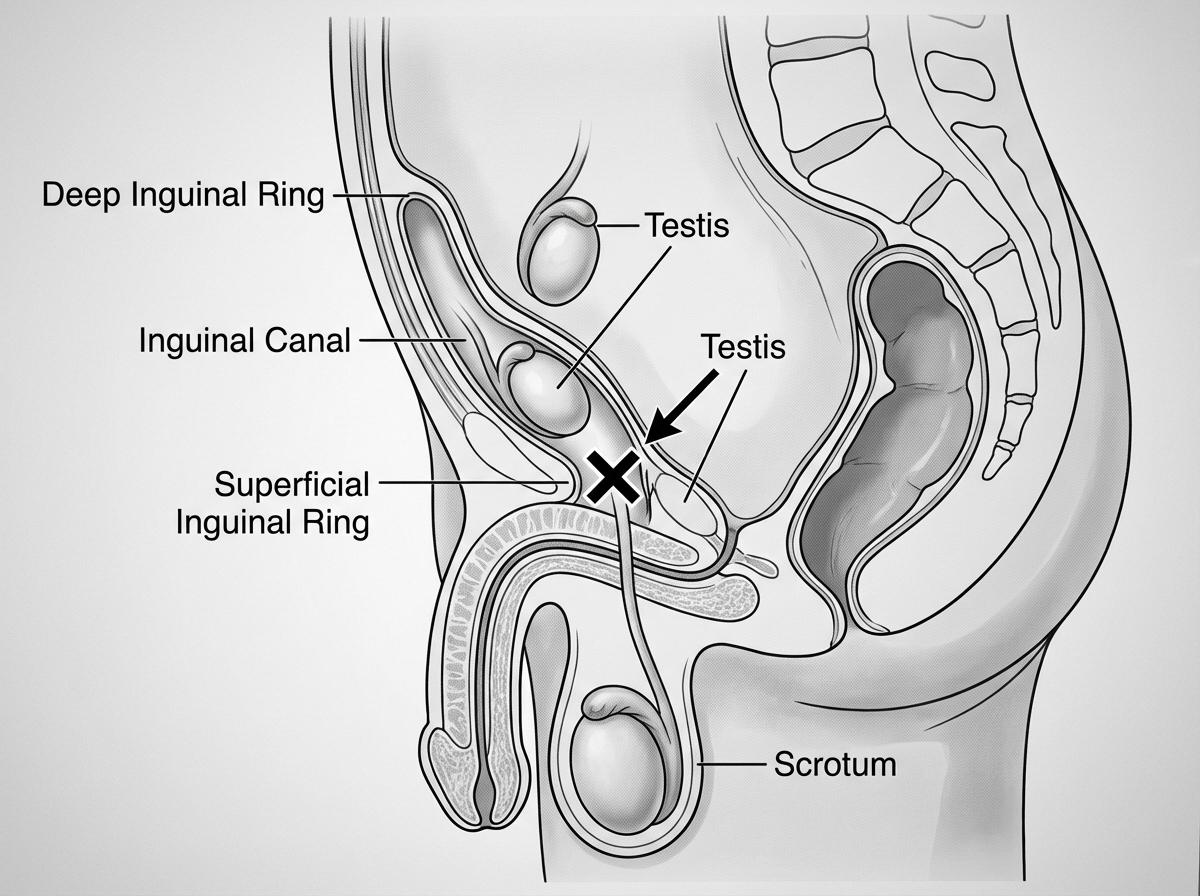
The testis reaches the point marked $X$ (the superficial inguinal ring) at which month of gestation? (Recent NEET Pattern 2016-17)
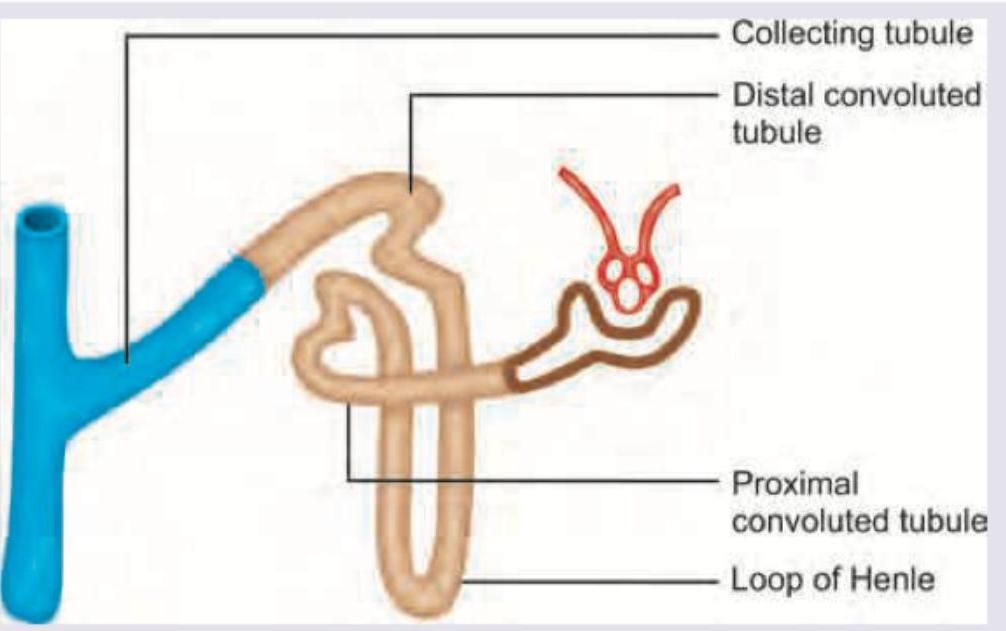
The part of the collecting duct system marked in blue develops from:
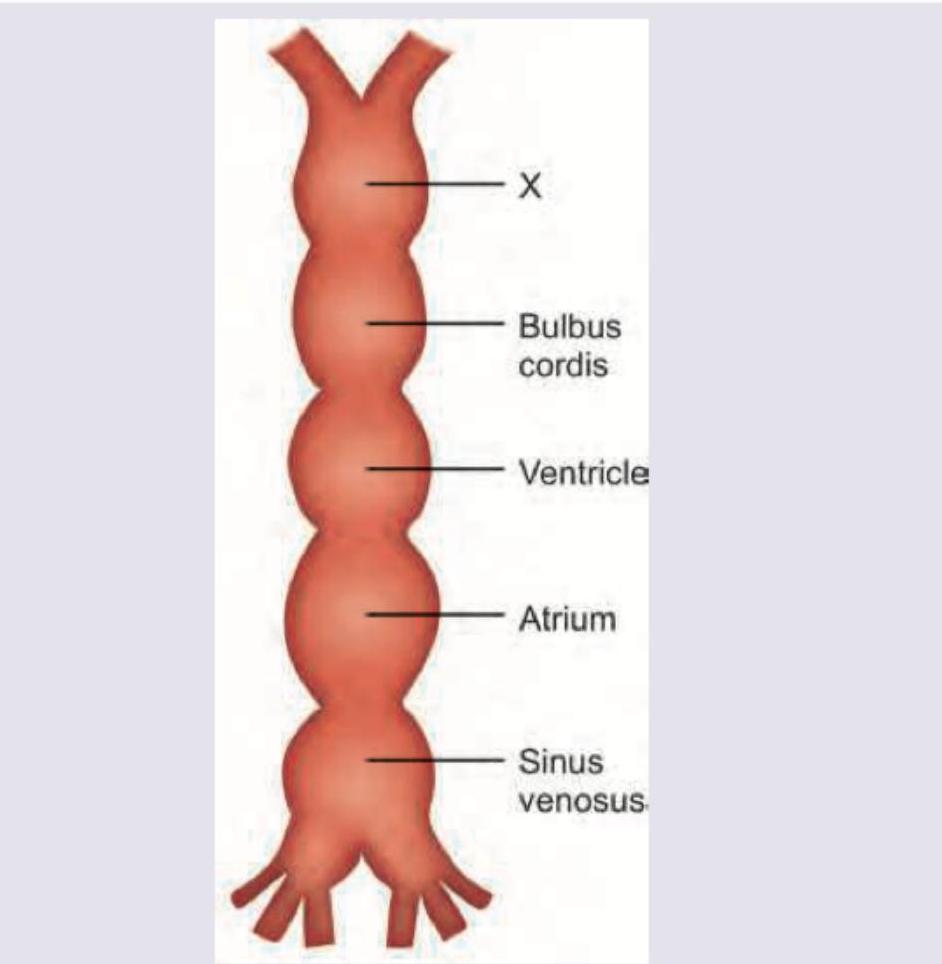
Identify the part shown as X in the primitive heart tube
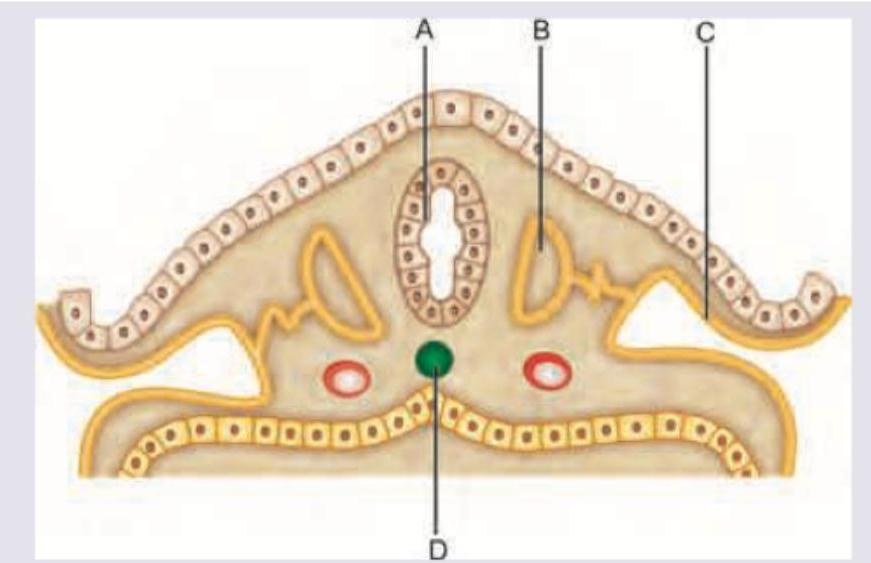
Which is correct about the diagram shown?
Which of the following is correct for the image shown below?
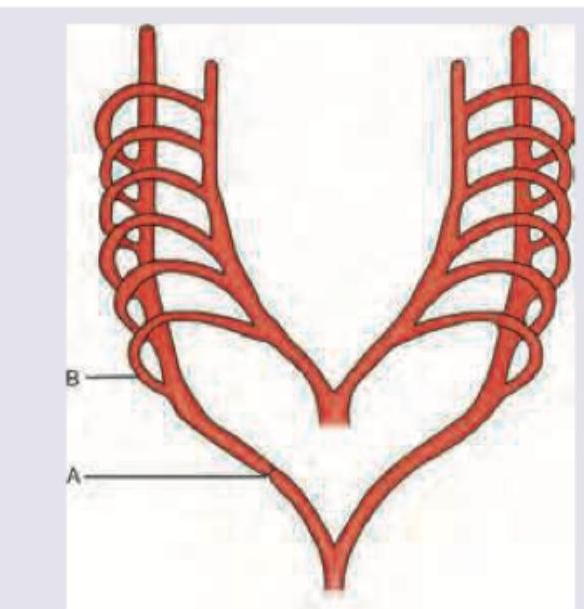
As shown in the figure, abnormal subclavian artery develops as a result of: (AIIMS May 2016)
Practice by Chapter
Gametogenesis and Fertilization
Practice Questions
Early Embryonic Development
Practice Questions
Placentation
Practice Questions
Development of Nervous System
Practice Questions
Development of Cardiovascular System
Practice Questions
Development of Gastrointestinal System
Practice Questions
Development of Urogenital System
Practice Questions
Development of Musculoskeletal System
Practice Questions
Development of Head and Neck
Practice Questions
Congenital Anomalies
Practice Questions
Teratology
Practice Questions
Molecular Mechanisms in Development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app