
Embryology and Development — MCQs

On this page
What is the chromosomal complement of a primary oocyte?
A newborn baby who was apparently healthy at birth develops aspiration pneumonia in the first two days of life. All attempts to feed the infant cause it to cough and choke. Which of the following abnormalities is the most likely cause of the infant's difficulties?
A branchial cyst arises due to which of the following embryological events?
What does the paramesonephric duct remain as in males?
The internal carotid artery is a derivative of which pharyngeal arch?
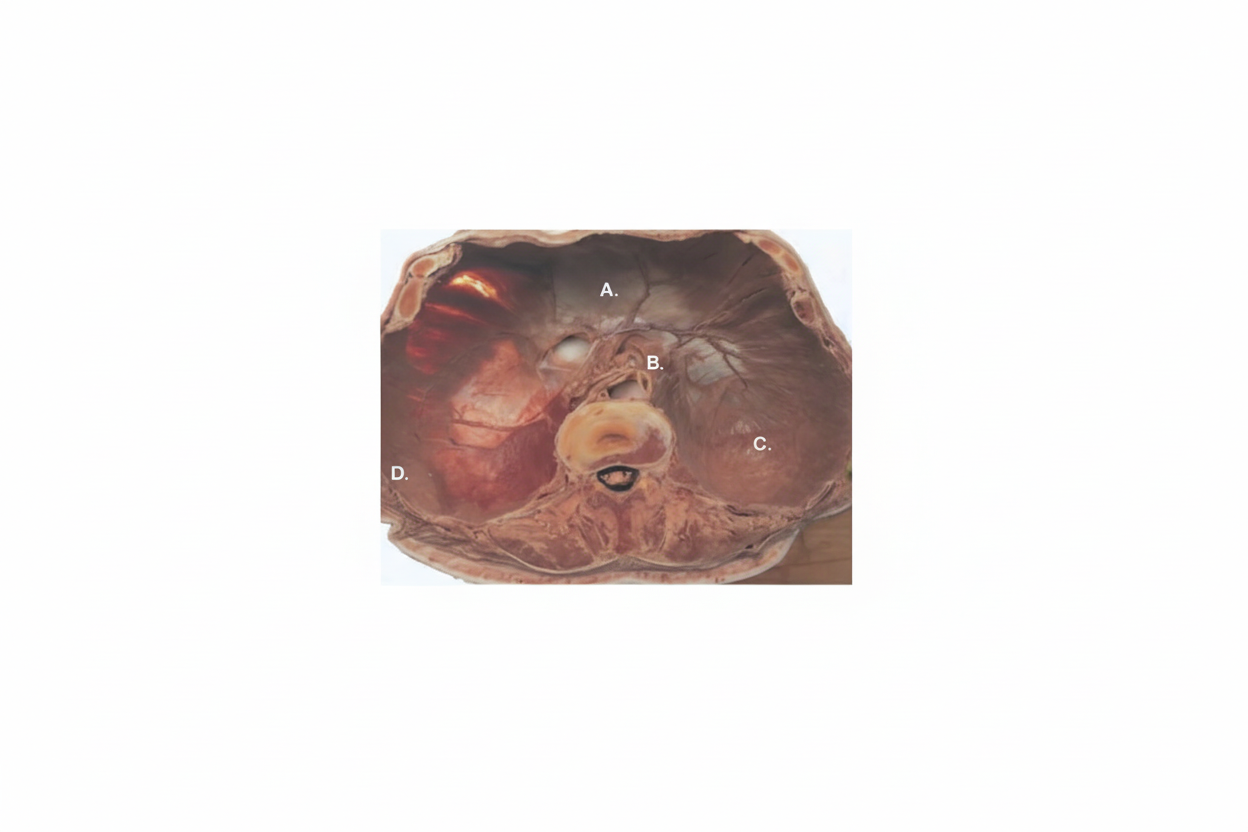
A neonate, within 4 hours of birth, presented with severe respiratory distress. He appears to be dyspneic, tachypneic, and cyanotic with severe retractions of the chest. On examination, grunting is present along with the use of accessory muscles. The neonate also appears to have a scaphoid abdomen and increased chest wall diameter. There is evidence of a shift of the point of maximal cardiac impulse from its original location to the right side. Chest x-ray of the neonate shows a defect in the development of which part of the responsible structure, causing this condition?
Cochlear function in the fetus develops between which gestational weeks?
Which of the following is NOT one of the phases of implantation of the embryo?
A double aortic arch is due to persistent?
A 5-day-old male infant is diagnosed with Hirschsprung disease. CT scan examination reveals an abnormally dilated colon. Which of the following is the most likely embryologic mechanism responsible for Hirschsprung disease?
Practice by Chapter
Gametogenesis and Fertilization
Practice Questions
Early Embryonic Development
Practice Questions
Placentation
Practice Questions
Development of Nervous System
Practice Questions
Development of Cardiovascular System
Practice Questions
Development of Gastrointestinal System
Practice Questions
Development of Urogenital System
Practice Questions
Development of Musculoskeletal System
Practice Questions
Development of Head and Neck
Practice Questions
Congenital Anomalies
Practice Questions
Teratology
Practice Questions
Molecular Mechanisms in Development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app