
Embryology and Development — MCQs

On this page
What is the function of the zona pellucida?
Which of the following masses develops along the lines of embryological fusion in the floor of the mouth?
At which stage does the conceptus reach the uterine cavity?
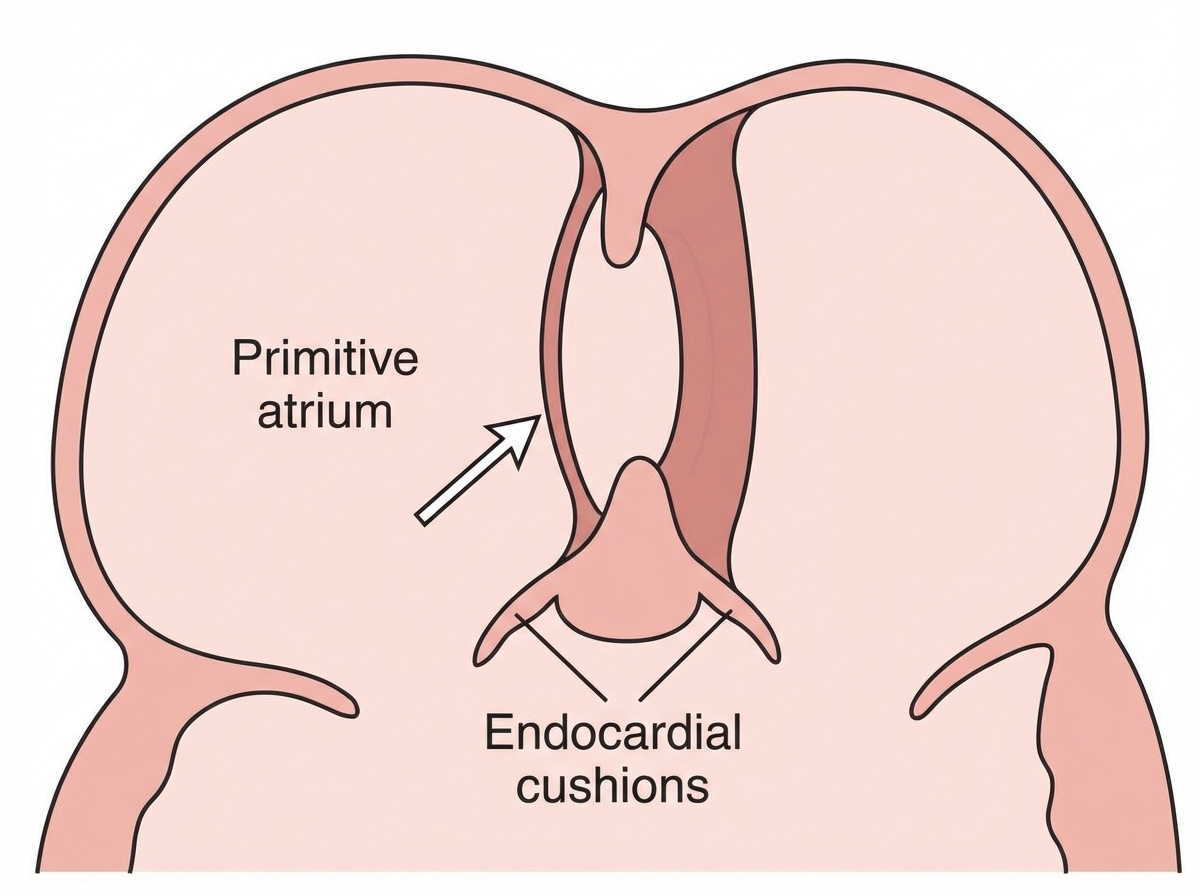
The marked area (valve of the foramen ovale) develops from:
The pancreas is derived from which embryonic structure?
The gastrosplenic ligament is derived from which of the following embryonic developmental structures?
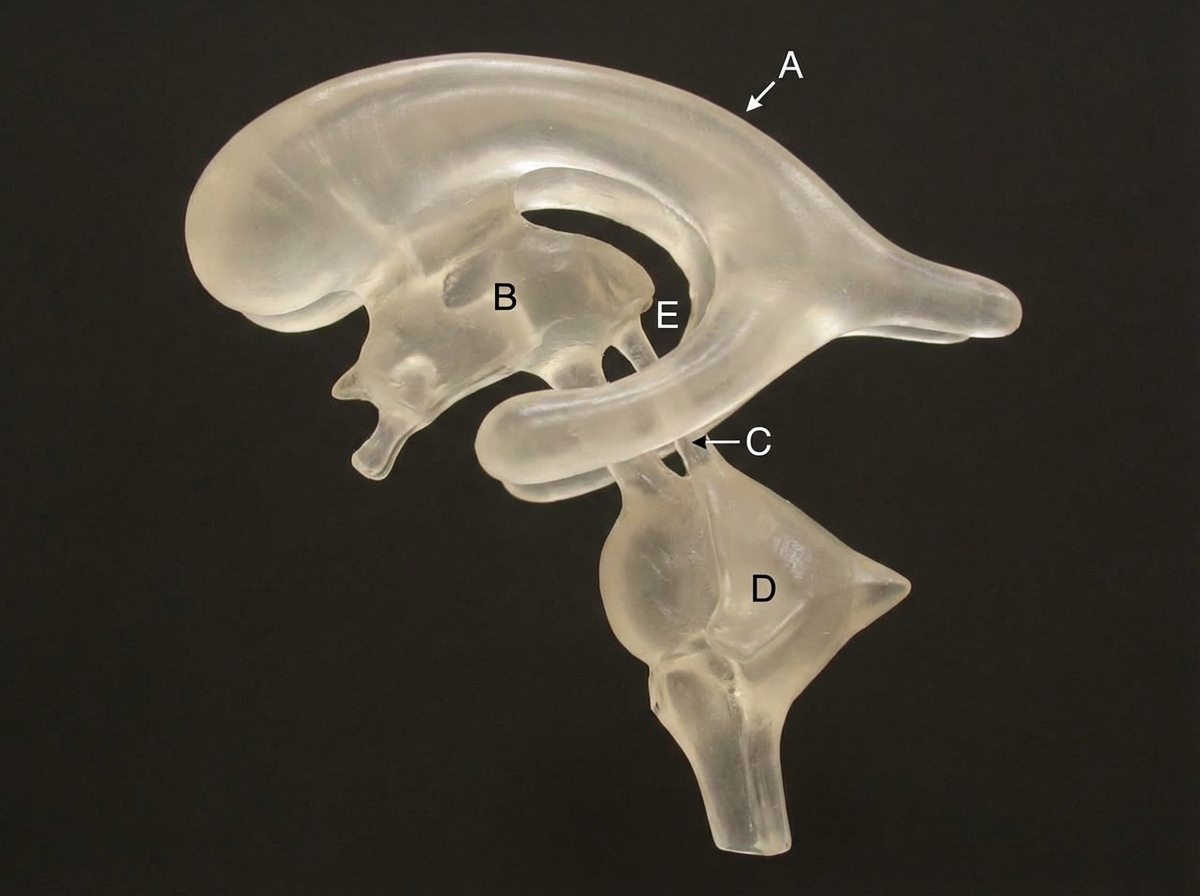
A neonate has suffered from a teratogenic insult during embryonic growth that has affected the mesencephalic part of his developing neural tube. In the presented cast of his ventricular system (left lateral view), which of the following areas might have suffered?
Allanto-enteric diverticulum is formed by the outgrowth of?
A patient with genotype X0 will have which of the following phenotypes, except?
What is your diagnosis?

Practice by Chapter
Gametogenesis and Fertilization
Practice Questions
Early Embryonic Development
Practice Questions
Placentation
Practice Questions
Development of Nervous System
Practice Questions
Development of Cardiovascular System
Practice Questions
Development of Gastrointestinal System
Practice Questions
Development of Urogenital System
Practice Questions
Development of Musculoskeletal System
Practice Questions
Development of Head and Neck
Practice Questions
Congenital Anomalies
Practice Questions
Teratology
Practice Questions
Molecular Mechanisms in Development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app