
Embryology and Development — MCQs

On this page
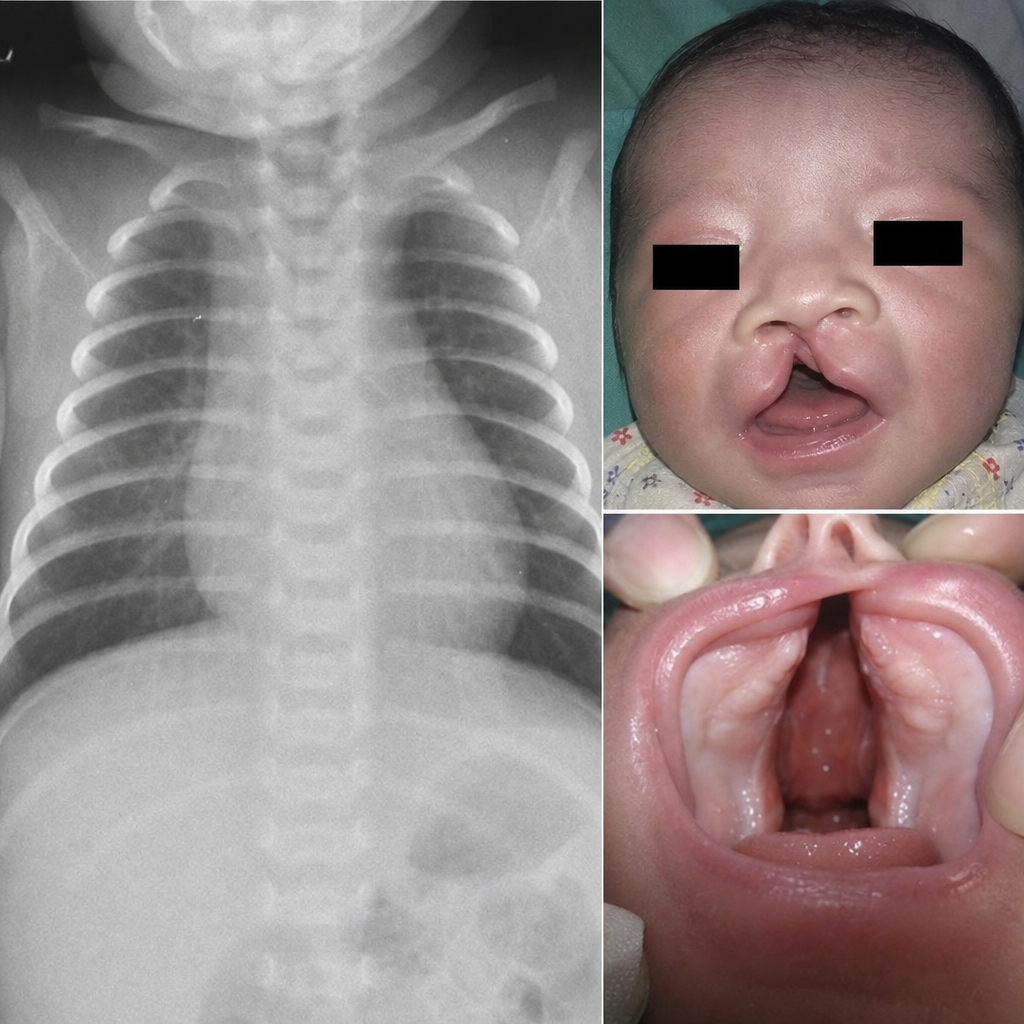
A newborn presents with recurrent seizures and cyanosis. Physical examination reveals characteristic facial abnormalities and chest x-ray findings as depicted. Which migratory cell population is principally responsible for the craniofacial and conotruncal abnormalities seen in this clinical scenario?
Which of the following statements is false regarding the notochord?
What is the probable diagnosis for a cyst in a child that is located at and associated with vertebral defects?
Which of the following structures is derived from the diencephalon?
Embryological development of the human vertebra is derived from which structure?
Ciliary muscles develop from which germ layer/cell type?
The crystalline lens is derived embryologically from which structure?
In which of the following conditions is a Barr body absent?
Which of the following structures is NOT derived from the first pharyngeal arch?
The round ligament of the uterus is derived from which embryonic structure?
Practice by Chapter
Gametogenesis and Fertilization
Practice Questions
Early Embryonic Development
Practice Questions
Placentation
Practice Questions
Development of Nervous System
Practice Questions
Development of Cardiovascular System
Practice Questions
Development of Gastrointestinal System
Practice Questions
Development of Urogenital System
Practice Questions
Development of Musculoskeletal System
Practice Questions
Development of Head and Neck
Practice Questions
Congenital Anomalies
Practice Questions
Teratology
Practice Questions
Molecular Mechanisms in Development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app