
Embryology and Development — MCQs

On this page
Defect in any of the following may result in renal agenesis, except:
Newborn babies are able to breathe and suck simultaneously due to which anatomical feature?
A newborn presents with cyanosis in the first week of life. The mother has a history of Diabetes. Chest X-ray findings and further investigations suggest that the symptoms are due to inappropriate circulation of oxygenated and deoxygenated blood between the body and the lungs. Survival in the neonatal period in such cases is facilitated by the foramen ovale and the ductus arteriosus, which permit some mixing of oxygenated and deoxygenated blood. What is the most likely diagnosis and the corresponding cardiac defect?
Closure of the foramen primum results from fusion of which of the following structures?
Failure of the intestinal loops to return to the abdominal cavity by week 11 after physiological hernia at the 6th week results in the formation of which condition?
All of the following develop from the Wolffian duct except:
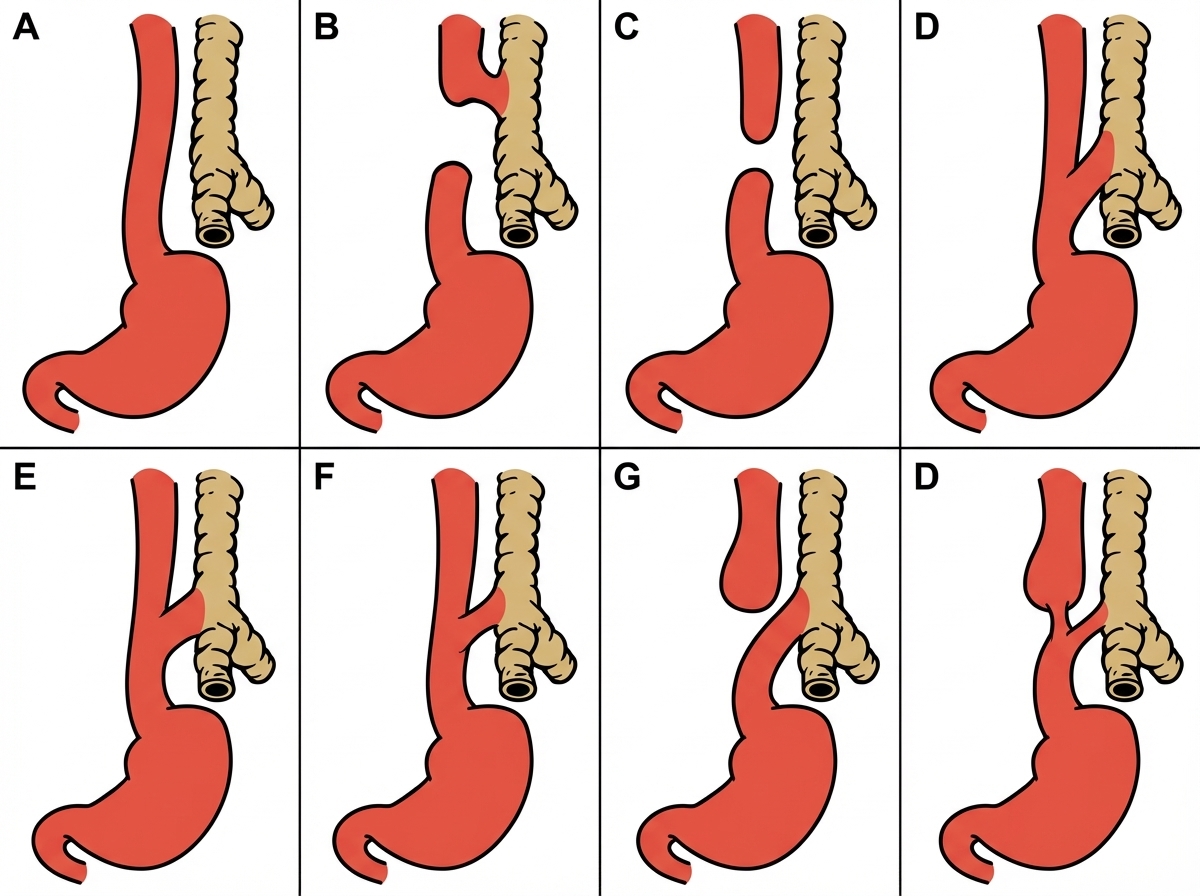
Shortly after birth, an infant develops abdominal distention and begins to drool. When she is given her first feeding, it runs out the side of her mouth, and she coughs and chokes. Physical examination reveals tachypnea, intercostal retractions, and bilateral pulmonary rales. Which esophageal anomaly most commonly causes these signs and symptoms?
All of the following are ectodermal derivatives EXCEPT?
At what gestational age do spontaneous fetal movements typically begin?
Which of the following is true regarding annular pancreas?
Practice by Chapter
Gametogenesis and Fertilization
Practice Questions
Early Embryonic Development
Practice Questions
Placentation
Practice Questions
Development of Nervous System
Practice Questions
Development of Cardiovascular System
Practice Questions
Development of Gastrointestinal System
Practice Questions
Development of Urogenital System
Practice Questions
Development of Musculoskeletal System
Practice Questions
Development of Head and Neck
Practice Questions
Congenital Anomalies
Practice Questions
Teratology
Practice Questions
Molecular Mechanisms in Development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app