
Embryology and Development — MCQs

On this page
The caecum is found to be placed below the stomach and in the midline. Which of the following abnormalities must have taken place during the rotation of the gut?
Karyotyping of the fetus may be done from all of the following except:
Which of the following respiratory structures is derived from the neural crest?
The human placenta is best described as:
Which embryonic structure forms first?
Cardiac looping in a fetus occurs on which day of gestation?
A person showing two cell lines derived from two different zygotes is known as?
Which is the first bone to ossify in the human body?
Which of the following structures does NOT contribute to the development of the tongue?
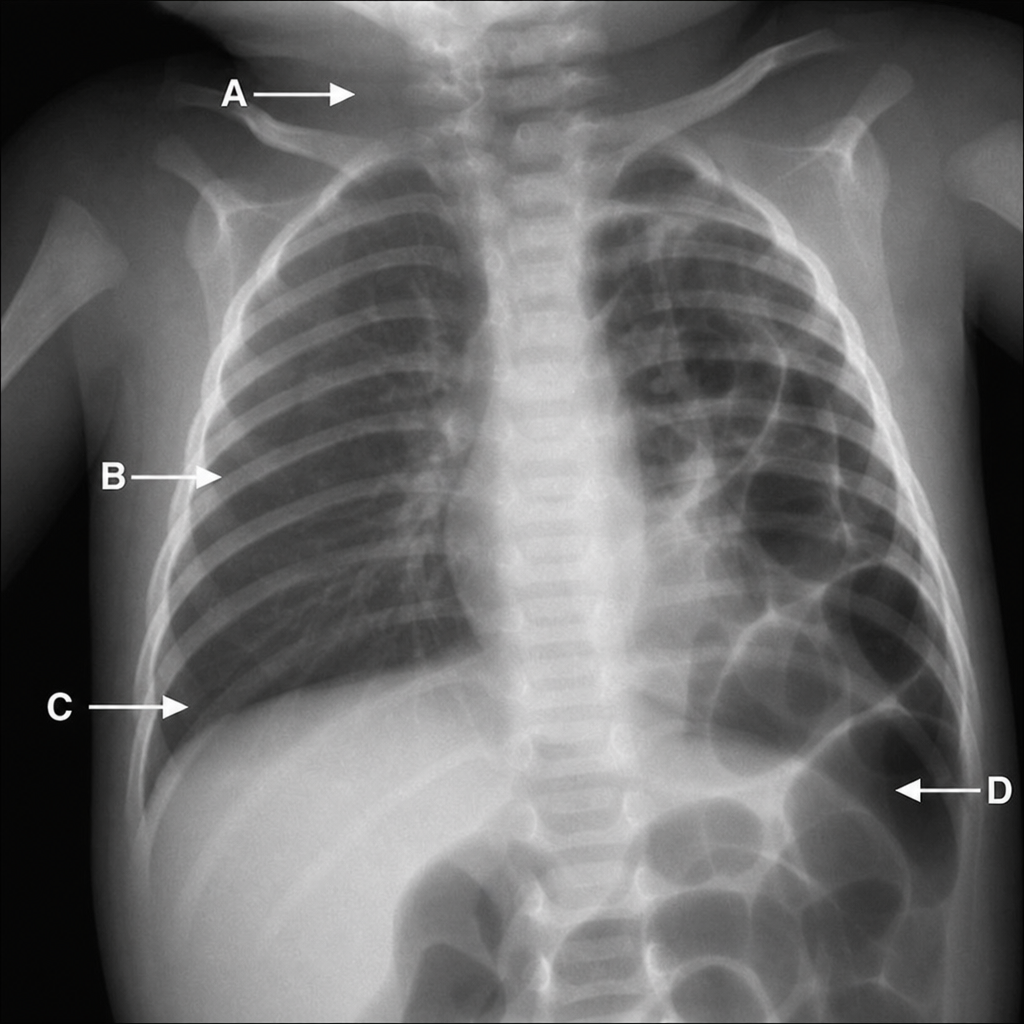
Which of the following markers indicates the site of a Bochdalek hernia?
Practice by Chapter
Gametogenesis and Fertilization
Practice Questions
Early Embryonic Development
Practice Questions
Placentation
Practice Questions
Development of Nervous System
Practice Questions
Development of Cardiovascular System
Practice Questions
Development of Gastrointestinal System
Practice Questions
Development of Urogenital System
Practice Questions
Development of Musculoskeletal System
Practice Questions
Development of Head and Neck
Practice Questions
Congenital Anomalies
Practice Questions
Teratology
Practice Questions
Molecular Mechanisms in Development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app