
Embryology and Development — MCQs

On this page
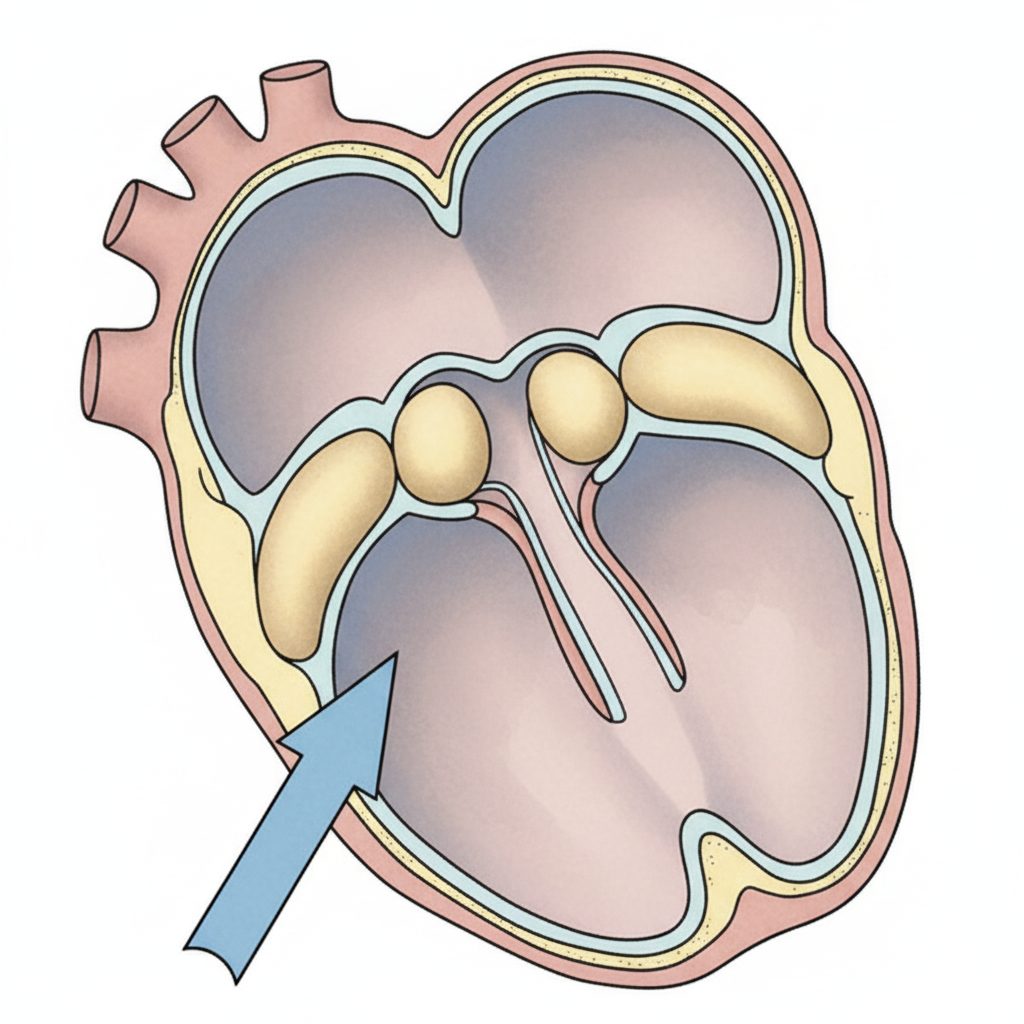
The structure marked by the blue arrow develops from which of the following structures?
Which of the following statements is true of cardiac development?
First evidence of primordial follicles can be seen in the ovaries at what stage of development?
Edwards syndrome is characterized by which chromosomal abnormality?
Which of the following is NOT a derivative of the paramesonephric duct?
In the testis, in which stage are haploid chromosomes present?
The fetus born during the 6th month of intrauterine life will NOT be able to survive due to which of the following reasons?
A 4-year-old child presents with fewer teeth than expected and lateral incisors exhibiting bifurcated roots with two root canals. What is this condition called?
The paramesonephric duct develops into which of the following structures?
Which of the following statements about Horseshoe kidney is true?
Practice by Chapter
Gametogenesis and Fertilization
Practice Questions
Early Embryonic Development
Practice Questions
Placentation
Practice Questions
Development of Nervous System
Practice Questions
Development of Cardiovascular System
Practice Questions
Development of Gastrointestinal System
Practice Questions
Development of Urogenital System
Practice Questions
Development of Musculoskeletal System
Practice Questions
Development of Head and Neck
Practice Questions
Congenital Anomalies
Practice Questions
Teratology
Practice Questions
Molecular Mechanisms in Development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app