
Embryology and Development — MCQs

On this page
Pulmonary veins develop from which embryonic structure?
In a complete cleft palate, the hard palate is totally separated from which structure?
From which germ layer do ameloblasts develop?
Around which structure does the rotation of the midgut loop occur?
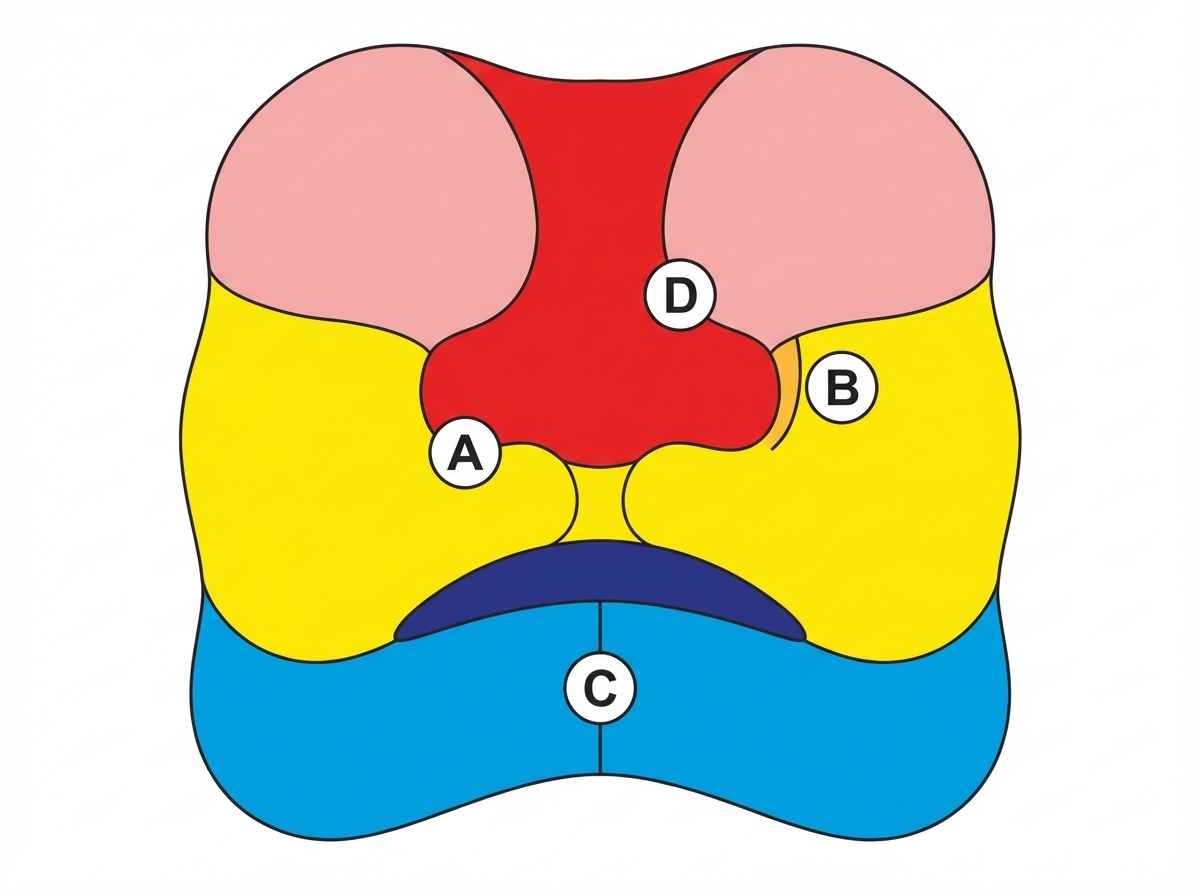
Failure of fusion of which of the following facial ridges results in the formation of an oblique facial cleft, leading to failure of nasolacrimal duct formation?
At what stage of embryonic development does an embryo normally begin to implant in the endometrium?
Which of the following is not a constituent of the umbilical cord?
Which of the following is NOT a derivative of the hindgut?
Which statement is true regarding the anal membrane?
Which of the following structures is derived from the telencephalon?
Practice by Chapter
Gametogenesis and Fertilization
Practice Questions
Early Embryonic Development
Practice Questions
Placentation
Practice Questions
Development of Nervous System
Practice Questions
Development of Cardiovascular System
Practice Questions
Development of Gastrointestinal System
Practice Questions
Development of Urogenital System
Practice Questions
Development of Musculoskeletal System
Practice Questions
Development of Head and Neck
Practice Questions
Congenital Anomalies
Practice Questions
Teratology
Practice Questions
Molecular Mechanisms in Development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app