
Embryology and Development — MCQs

On this page
True regarding the umbilical cord?
Diplotene and zygotene stages are seen in which phase of cell division?
The diaphragm develops from all of the following structures except:
A 25-day-old neonate presented with cyanosis, sweating, and difficulty in feeding. There is a history of the mother taking some drug in the first trimester for her bipolar disease. On examination, a holosystolic murmur is heard parasternally in the left 4th intercostal space, which increased on inspiration. S3 and S4 heart sounds are present. Which embryological remnant is associated with this condition?
Ribs are developed from which embryonic structure?
A newborn baby has projectile vomiting shortly after each feeding. Investigations reveal obstruction of the digestive tract due to an annular pancreas. Annular pancreas is an abnormality in which of the following developmental processes?
DiGeorge syndrome is due to a defect in which pharyngeal pouch?
The corona radiata of the ovum is formed from which of the following?
When does the metanephros become functional?
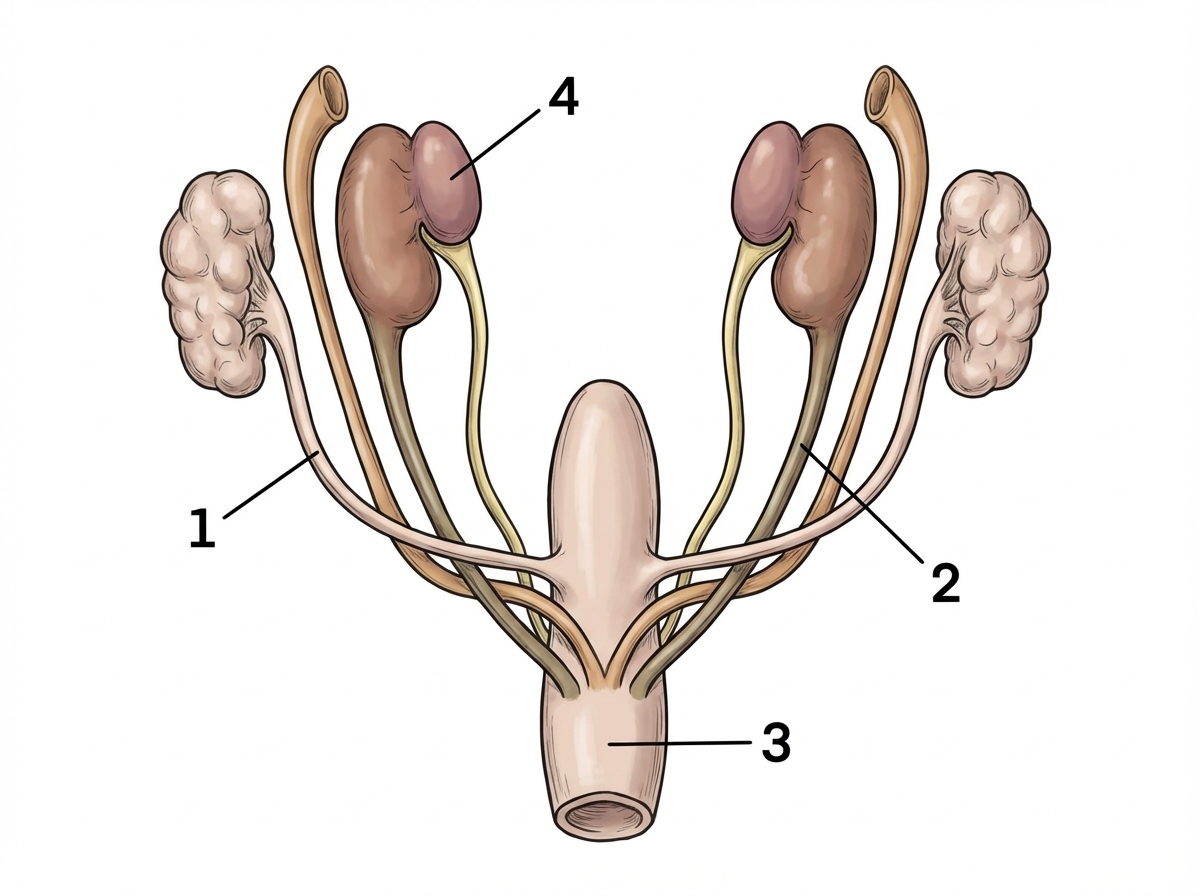
Which of the following statements regarding the developmental origin of the urogenital system is WRONG?
Practice by Chapter
Gametogenesis and Fertilization
Practice Questions
Early Embryonic Development
Practice Questions
Placentation
Practice Questions
Development of Nervous System
Practice Questions
Development of Cardiovascular System
Practice Questions
Development of Gastrointestinal System
Practice Questions
Development of Urogenital System
Practice Questions
Development of Musculoskeletal System
Practice Questions
Development of Head and Neck
Practice Questions
Congenital Anomalies
Practice Questions
Teratology
Practice Questions
Molecular Mechanisms in Development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app