
Embryology and Development — MCQs

On this page
What structure does the vitelline vein form?
Lanugo hair appears at:
Chromosome 21 belongs to which of the following subtypes?
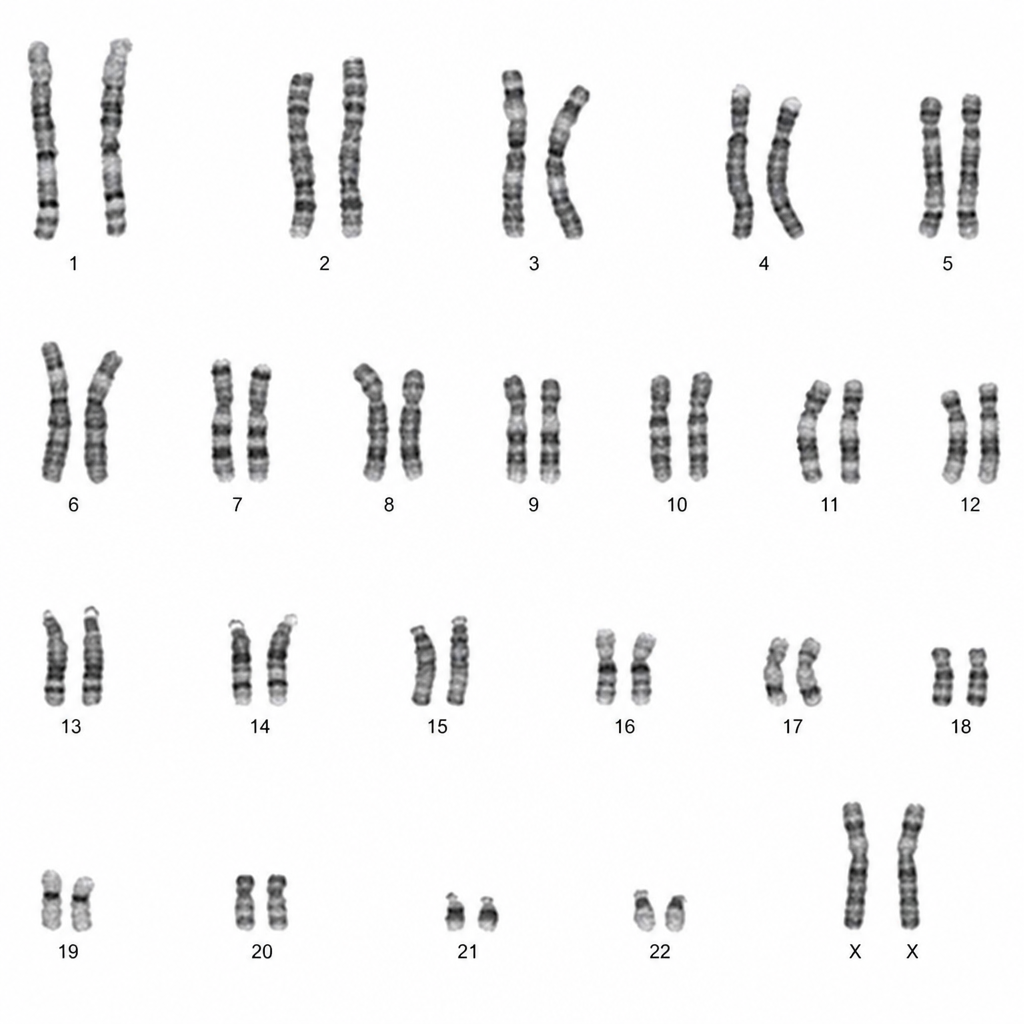
The chromosomal mapping is suggestive of which of the following conditions?
Which of the following is not a neural crest derivative?
A 1-day-old infant has a mass protruding through her umbilicus. Physical examination reveals an umbilical hernia. A CT scan reveals that part of another organ is attached to the inner surface of the hernia. What portion of the gastrointestinal tract is most likely to be attached to the inner surface of the umbilical hernia?
Which of the following structures is not involved in the development of the diaphragm?
A collaural fistula is described as:
A newborn baby presents with a left unilateral cleft lip and an intact palate. Which of the following developmental defects best explains this condition?
What is the nature of the covering over an omphalocele?
Practice by Chapter
Gametogenesis and Fertilization
Practice Questions
Early Embryonic Development
Practice Questions
Placentation
Practice Questions
Development of Nervous System
Practice Questions
Development of Cardiovascular System
Practice Questions
Development of Gastrointestinal System
Practice Questions
Development of Urogenital System
Practice Questions
Development of Musculoskeletal System
Practice Questions
Development of Head and Neck
Practice Questions
Congenital Anomalies
Practice Questions
Teratology
Practice Questions
Molecular Mechanisms in Development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app