
Embryology and Development — MCQs

On this page
All are derivatives of ectoderm except?
What is a female pseudohermaphrodite?
Which of the following is untrue regarding ectodermal clefts?
The mandible is embryologically derived from which structure?
Embryologically, the forehead develops from which of the following structures?
Which mesodermal component gives rise to the muscular component of the dorsal aorta?
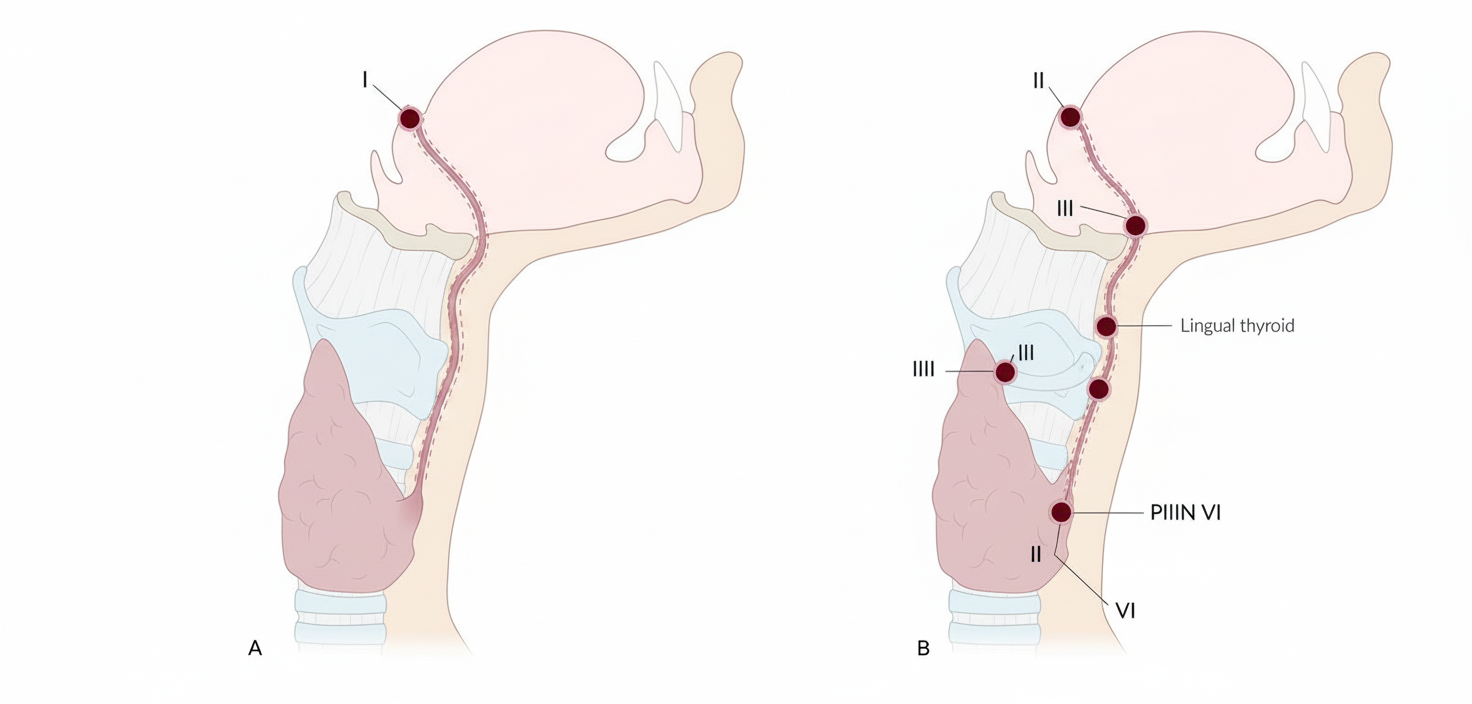
The diagram represents the path traversed in the neck by the developing thyroid gland embryo. Which point along this path is the commonest site of a thyroglossal cyst?
Trisomy 13 is also known as which syndrome?
A 4-year-old male child is admitted to the hospital with severe vomiting. Radiographic examination and history taking reveals that the boy suffers from an annular pancreas. Which of the following structures is most typically obstructed by this condition?
A 3-month-old infant's mother noticed that the iris of the baby's right eye was missing. Examination revealed a defect in the inferior region of the iris and pupillary region, giving it a characteristic keyhole appearance. Which of the following mechanisms during embryonic development will most likely lead to this condition?
Practice by Chapter
Gametogenesis and Fertilization
Practice Questions
Early Embryonic Development
Practice Questions
Placentation
Practice Questions
Development of Nervous System
Practice Questions
Development of Cardiovascular System
Practice Questions
Development of Gastrointestinal System
Practice Questions
Development of Urogenital System
Practice Questions
Development of Musculoskeletal System
Practice Questions
Development of Head and Neck
Practice Questions
Congenital Anomalies
Practice Questions
Teratology
Practice Questions
Molecular Mechanisms in Development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app