
Embryology and Development — MCQs

On this page
All of the following are derived from the second pharyngeal arch except?
Which of the following bones ossify first?
Which of the following is NOT a true statement regarding the derivatives of the aortic arches?
Which of the following statements is NOT true regarding paramedian pits?
The cecum is found to be placed below the stomach and is midline. Which of the following abnormalities must have taken place during the rotation of the gut?
The Glossopharyngeal nerve supplies the posterior 1/3 of the tongue because it develops from which embryological structure?
Polar bodies are formed during which process?
Ossification of long bones begins at what age?
The palatine tonsil develops from which of the following embryonic structures?
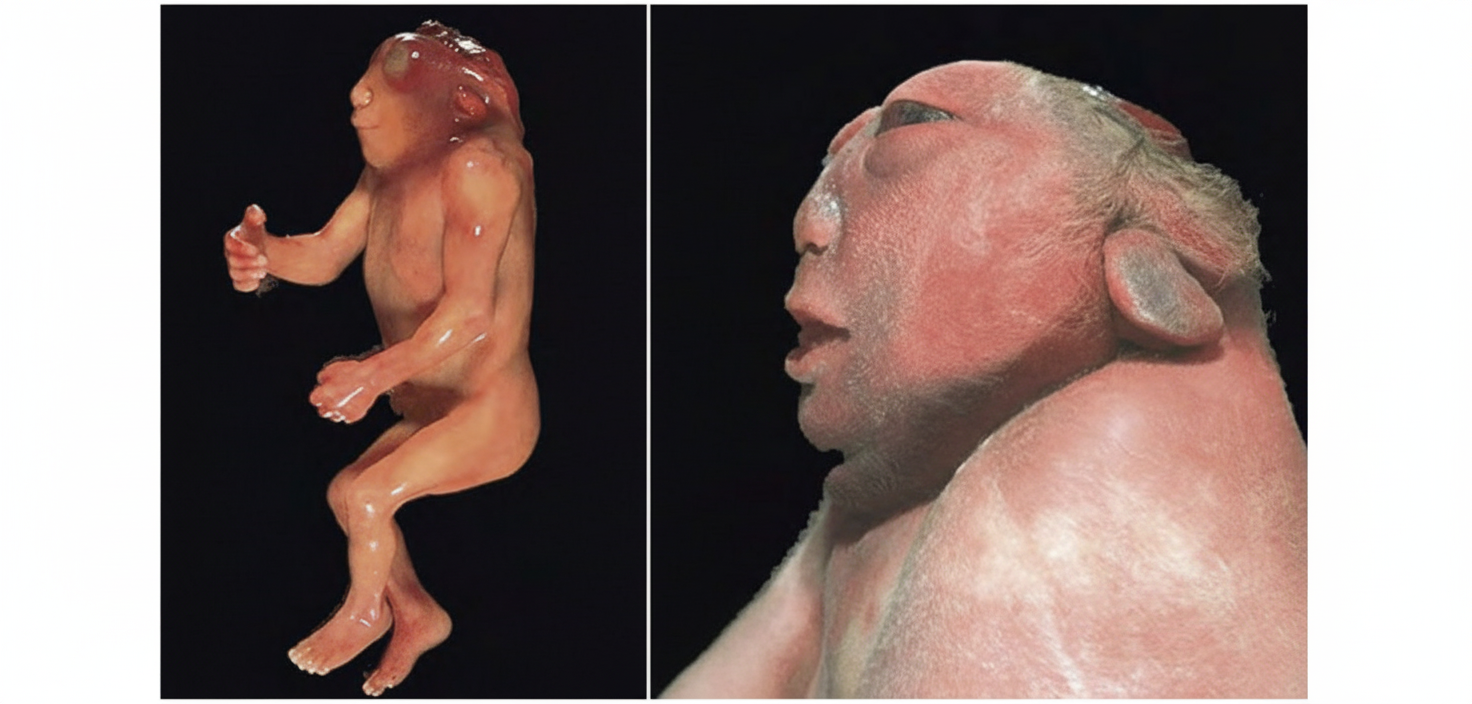
What is the name of the congenital anomaly this child is suffering from?
Practice by Chapter
Gametogenesis and Fertilization
Practice Questions
Early Embryonic Development
Practice Questions
Placentation
Practice Questions
Development of Nervous System
Practice Questions
Development of Cardiovascular System
Practice Questions
Development of Gastrointestinal System
Practice Questions
Development of Urogenital System
Practice Questions
Development of Musculoskeletal System
Practice Questions
Development of Head and Neck
Practice Questions
Congenital Anomalies
Practice Questions
Teratology
Practice Questions
Molecular Mechanisms in Development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app