
Embryology and Development — MCQs

On this page
The upper three-fourths of the vagina develops from which embryonic structure?
All of the following are components of the placental barrier, EXCEPT:
Which of the following procedures is used as a routine technique for karyotyping using light microscopy?
What is true about Lyonization of the X chromosome?
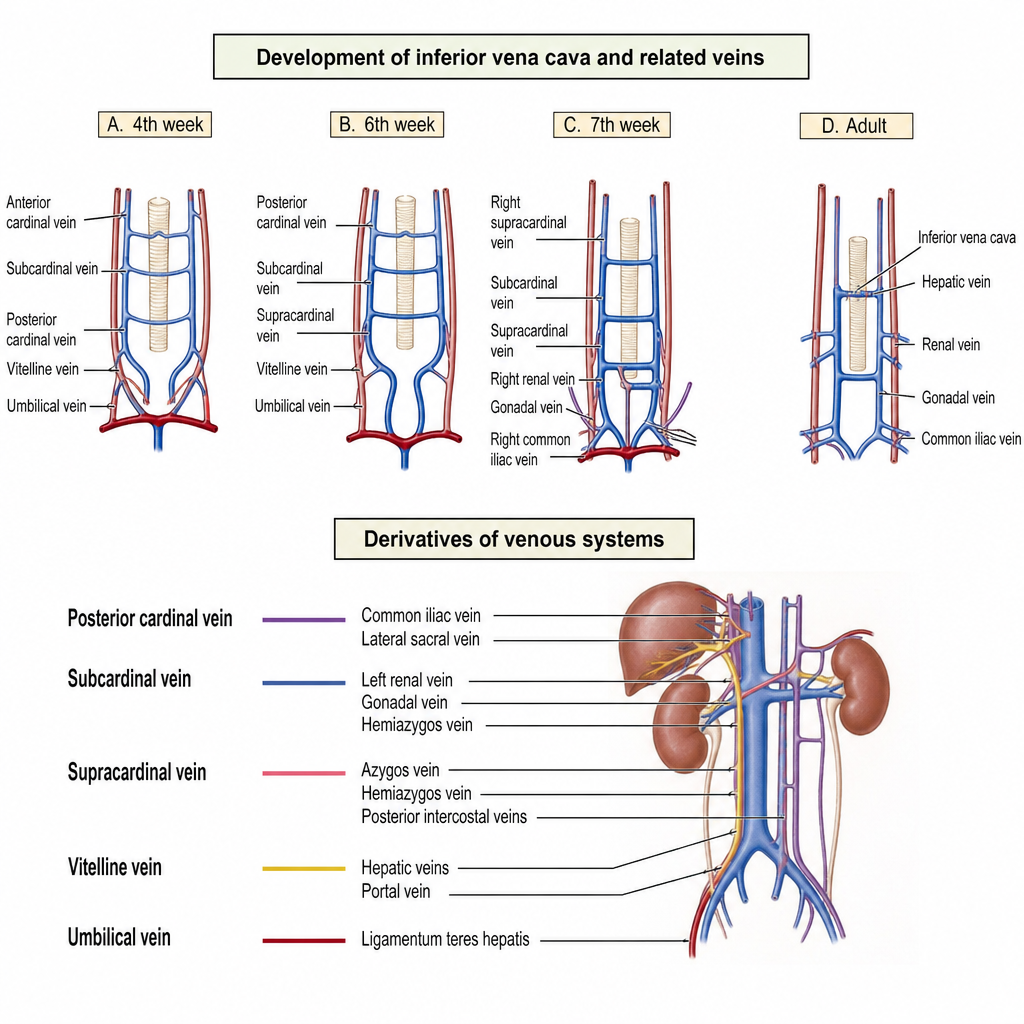
The Psoas Vein develops from which of these embryonic structures?
The presence of a uterus and fallopian tubes in an otherwise phenotypically normal male is due to which of the following?
Which of the following structures is derived from the ectoderm?
What is the normal composition of vessels within the umbilical cord?
Trophoblast gives rise to all of the following EXCEPT?
Persistence of the distal part of the vitellointestinal duct results in which of the following?
Practice by Chapter
Gametogenesis and Fertilization
Practice Questions
Early Embryonic Development
Practice Questions
Placentation
Practice Questions
Development of Nervous System
Practice Questions
Development of Cardiovascular System
Practice Questions
Development of Gastrointestinal System
Practice Questions
Development of Urogenital System
Practice Questions
Development of Musculoskeletal System
Practice Questions
Development of Head and Neck
Practice Questions
Congenital Anomalies
Practice Questions
Teratology
Practice Questions
Molecular Mechanisms in Development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app