
Embryology and Development — MCQs

On this page
Posterior one-third of the tongue develops from which embryonic structure?
The 4th aortic arch is responsible for the formation of which structure?
Which is the earliest system to become functional in a fetus?
Which among the following is a neural tube defect?
At what stage of development is an embryo termed a fetus, according to embryologists?
All of the following are derived from the pharyngeal arches except?
Which of the following is a congenital anomaly arising from the first branchial cleft?
In ectodermal dysplasia, all of the following structures are affected EXCEPT:
Which of the following developmental defects of the urogenital sinus NEVER occurs in the female?
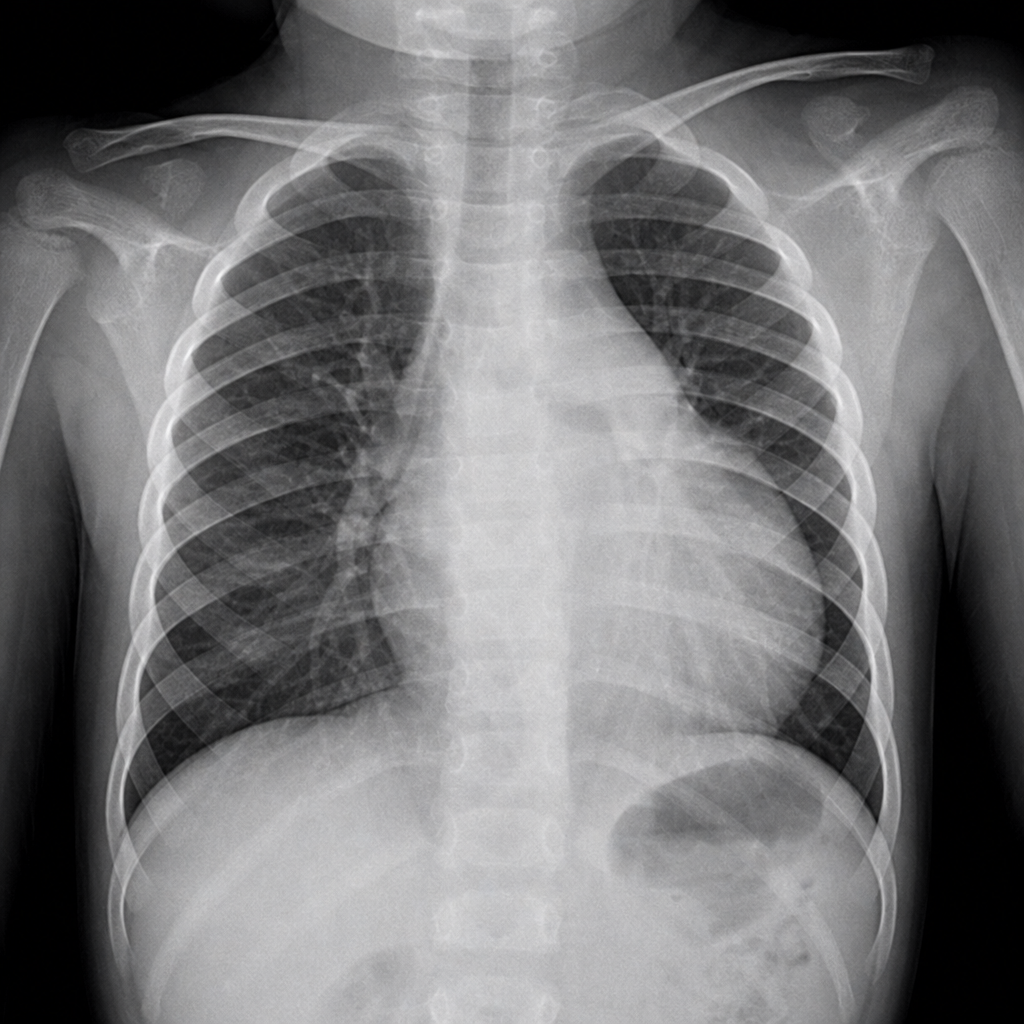
An 8-year-old boy presented with fever and cough. A chest X-ray was performed showing a right-sided cardiac apex and right-sided gastric bubble. Which of the following abnormalities in embryonic development could lead to findings such as those seen on the chest X-ray?
Practice by Chapter
Gametogenesis and Fertilization
Practice Questions
Early Embryonic Development
Practice Questions
Placentation
Practice Questions
Development of Nervous System
Practice Questions
Development of Cardiovascular System
Practice Questions
Development of Gastrointestinal System
Practice Questions
Development of Urogenital System
Practice Questions
Development of Musculoskeletal System
Practice Questions
Development of Head and Neck
Practice Questions
Congenital Anomalies
Practice Questions
Teratology
Practice Questions
Molecular Mechanisms in Development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app