
Embryology and Development — MCQs

On this page
During which fetal developmental stage do the testes descend into the scrotum?
The central tendon of the diaphragm is derived from which embryonic structure?
The embryo implants on the endometrium after how many days of fertilization?
Fertilization is complete when:
Cleft tongue and clefting of the mandibular alveolar process are seen in which of the following conditions?
What is the persistent remnant of the axial artery of the upper limb?
When a horseshoe kidney develops, the ascent of the kidney is restricted by which structure?
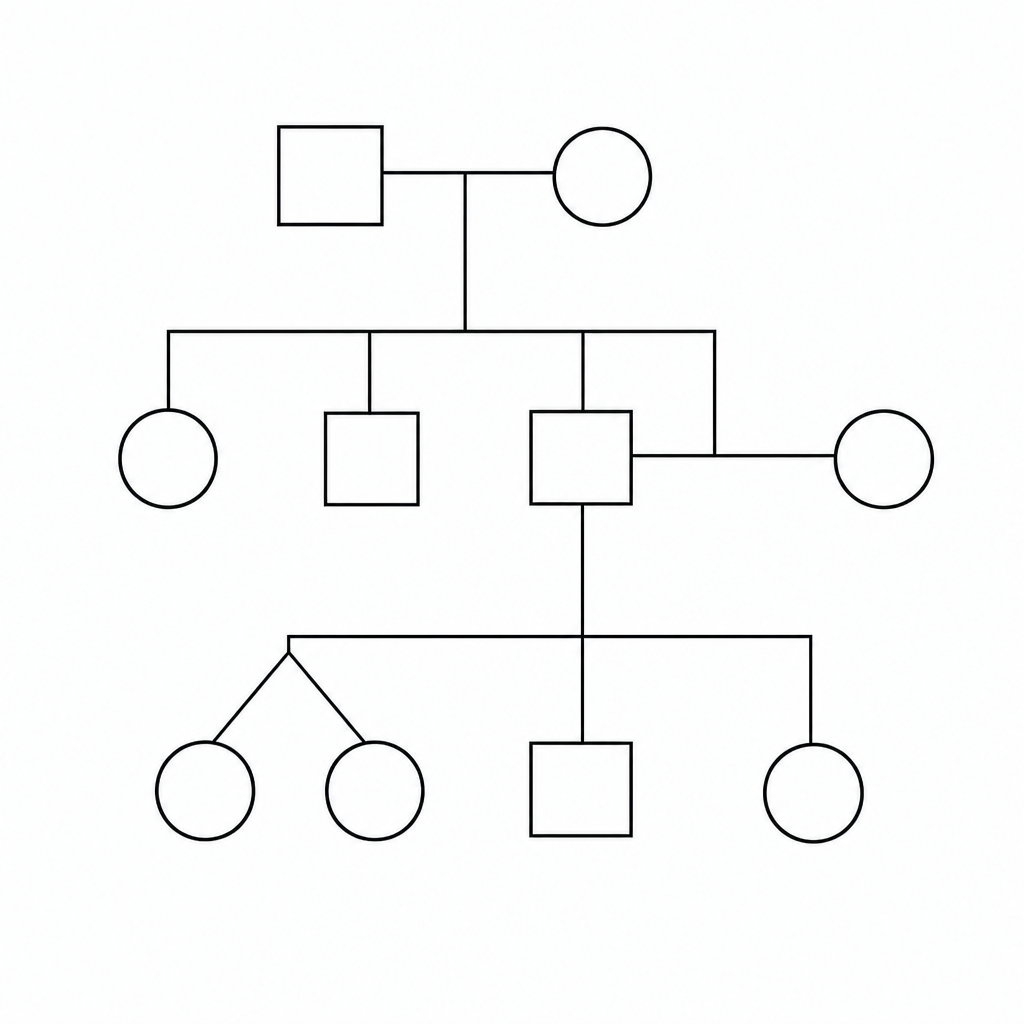
Which of the following is indicated by the pedigree given below?
Which of the following is NOT true regarding the development of the ovary?
Which of the following brainstem nuclei is not derived from the alar plate?
Practice by Chapter
Gametogenesis and Fertilization
Practice Questions
Early Embryonic Development
Practice Questions
Placentation
Practice Questions
Development of Nervous System
Practice Questions
Development of Cardiovascular System
Practice Questions
Development of Gastrointestinal System
Practice Questions
Development of Urogenital System
Practice Questions
Development of Musculoskeletal System
Practice Questions
Development of Head and Neck
Practice Questions
Congenital Anomalies
Practice Questions
Teratology
Practice Questions
Molecular Mechanisms in Development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app