
Embryology and Development — MCQs

On this page
A failure of fusion of the maxillary process with the medial nasal process during embryonic development results in which type of cleft anomaly?
A developmental remnant of the embryological hindgut persisting in the retrorectal (presacral) space is most likely to give rise to which of the following lesions?
Match each of the following organs with its correct embryological tissue of origin: Organ Embryological Origin A. Thyroid gland 1. Neural crest cells B. Adrenal medulla 2. Intermediate mesoderm C. Kidney 3. Endoderm
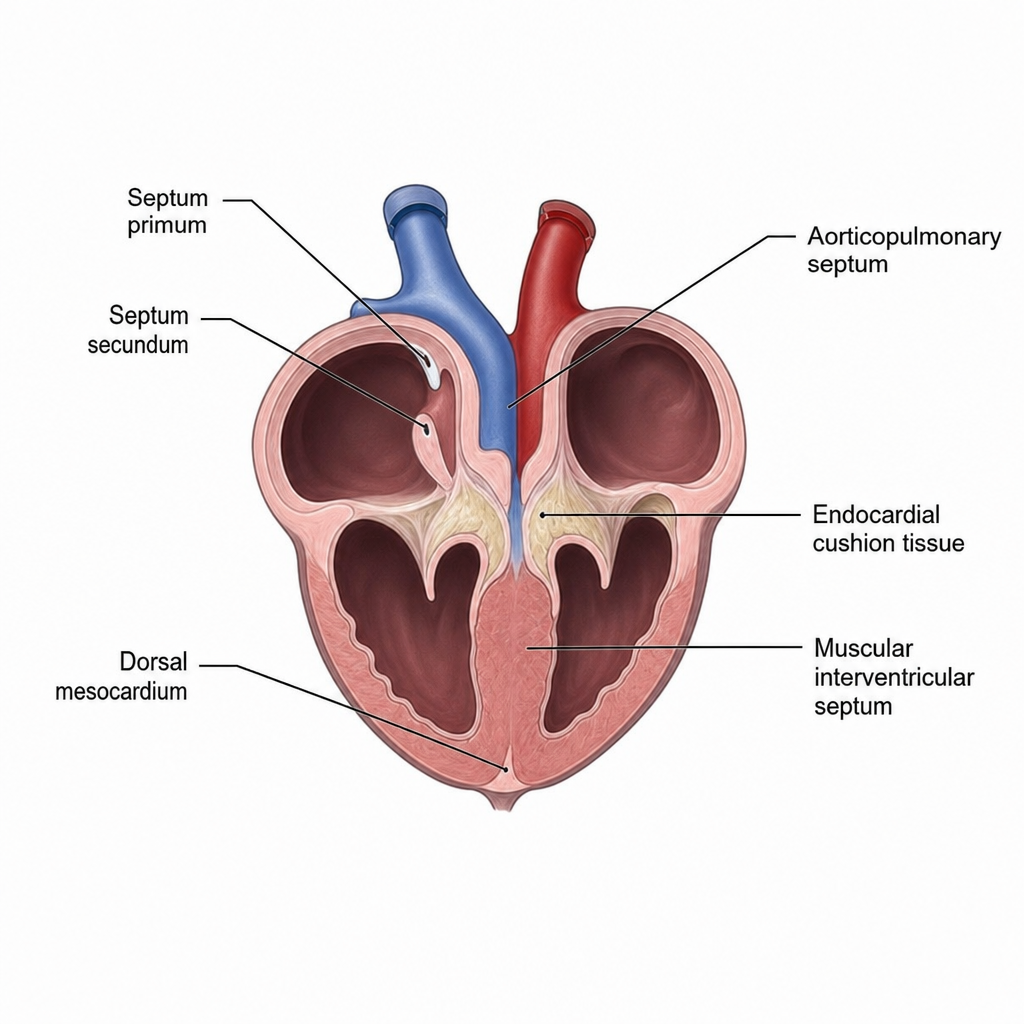
A neonate is noted to have a harsh pansystolic murmur loudest at the left lower sternal border. Echocardiography confirms the most common anatomical subtype of ventricular septal defect. The embryological schematic in Image 1 illustrates ventricular septation, with structures labeled but the site of defect not directly indicated. Which specific fusion event, if it fails to occur, results in the most common type of ventricular septal defect — and which labeled structure in the image represents the tissue that must fuse with the muscular interventricular septum to complete the membranous septum?
Evaluating a neonate with multiple congenital anomalies including cervical fistula draining mucus, thymic hypoplasia, and cardiac outflow tract defects, which phylogenetic developmental process has most likely been disrupted?
A genetic study reveals that a patient with congenital heart disease has abnormal neural crest cell migration. Comparing this to reptilian heart development, which specific cardiac structure's formation would be most affected?
Which embryonic structure in humans is homologous to the cloaca found in birds and reptiles?
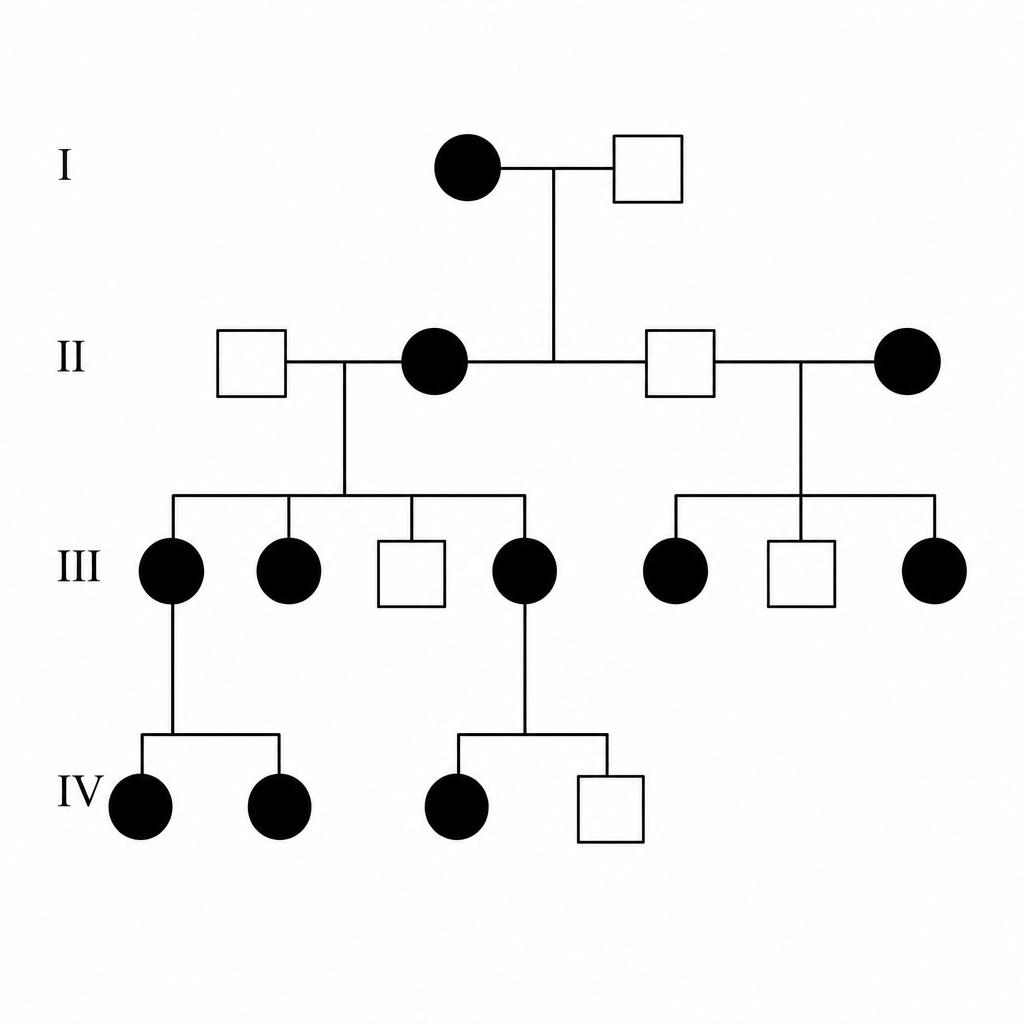
What is the pattern of inheritance shown in the given pedigree chart?
Maximum number of oogonia is seen at which stage?
What is the cause of hydrocele in infants?
Practice by Chapter
Gametogenesis and Fertilization
Practice Questions
Early Embryonic Development
Practice Questions
Placentation
Practice Questions
Development of Nervous System
Practice Questions
Development of Cardiovascular System
Practice Questions
Development of Gastrointestinal System
Practice Questions
Development of Urogenital System
Practice Questions
Development of Musculoskeletal System
Practice Questions
Development of Head and Neck
Practice Questions
Congenital Anomalies
Practice Questions
Teratology
Practice Questions
Molecular Mechanisms in Development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app