
Back — MCQs

On this page
All are pierced in Lumbar Puncture except:
A 7-year-old female who is somewhat obese is brought to the emergency department because of a soft lump above the buttocks. Upon physical examination you note the lump is located just superior to the iliac crest unilaterally on the left side. The protrusion is deep to the skin and pliable to the touch. Which of the following is the most probable diagnosis?
All are TRUE about intervertebral disc, EXCEPT:
Membrana tectoria is continuation of:
Which of the following parts of the vertebral canal shows the first secondary curve to develop?
After a 26-year-old man's car was sideswiped by a large truck, he is brought to the emergency department with multiple fractures of the transverse processes of the cervical and upper thoracic vertebrae. Which of the following muscles might be affected?
During a routine physical examination a 65-year-old male patient is tested for ease and flexibility of the movements of his lumbar region. Which of the following movements is most characteristic of the intervertebral joints in the lumbar region?
A 33-year-old man is brought to the emergency department after being involved in a major motor vehicle accident. He is unable to move his legs and complains of severe pain in his mid to lower back. On physical examination, he is found to have exquisite tenderness over some of the bony prominence of his lower back, but no gross physical deformity can be appreciated. On neurologic examination, flaccid paralysis of both lower extremities and complete anesthesia to all sensory modalities below approximately the L3 dermatome are noted. Catheterization of his bladder yields approximately 700 mL of urine. Plain radiographs of the spine reveal compression fracture in the body of L3 with greater than 50% of loss in its height. A computed tomography (CT) scan through this area reveals a burst fracture of the body of L3. There are large fragments of bone driven dorsally with an 80% canal compromise. What is the cause of weakness?
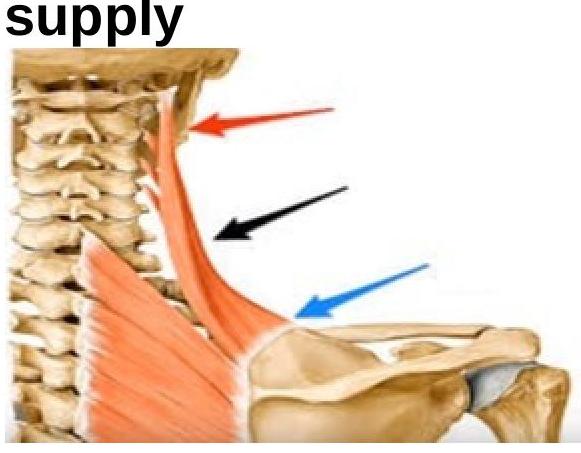
What is the principal nerve supply of the shown muscle among the following options?
Shape of trapezius muscle is:
Practice by Chapter
Vertebral Column
Practice Questions
Spinal Cord and Meninges
Practice Questions
Back Muscles and Fasciae
Practice Questions
Vertebral Joints and Ligaments
Practice Questions
Vasculature of the Back
Practice Questions
Innervation of the Back
Practice Questions
Clinical Aspects of Back Disorders
Practice Questions
Applied Anatomy of the Back
Practice Questions
Surface Anatomy of the Back
Practice Questions
Development of the Vertebral Column
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app