
Back — MCQs

On this page
A 32-year-old male elite athlete felt severe pain radiating to the posterior aspect of his right thigh and leg during an intense training session involving heavy weights. MRI revealed a ruptured L4/L5 intervertebral disk. Which nerve is most probably affected?
Which muscle, anatomically considered a back muscle, is functionally related to the thorax?
A 42-year-old woman with metastatic breast cancer is known to have tumors in the intervertebral foramina between the fourth and fifth cervical vertebrae and between the fourth and fifth thoracic vertebrae. Which of the following spinal nerves may be damaged?
Which ligament is the primary limitation to extension of the vertebral column?
Which of the following is NOT a flexor of the lumbar spine?
Which vertebra has the most prominent spinous process?
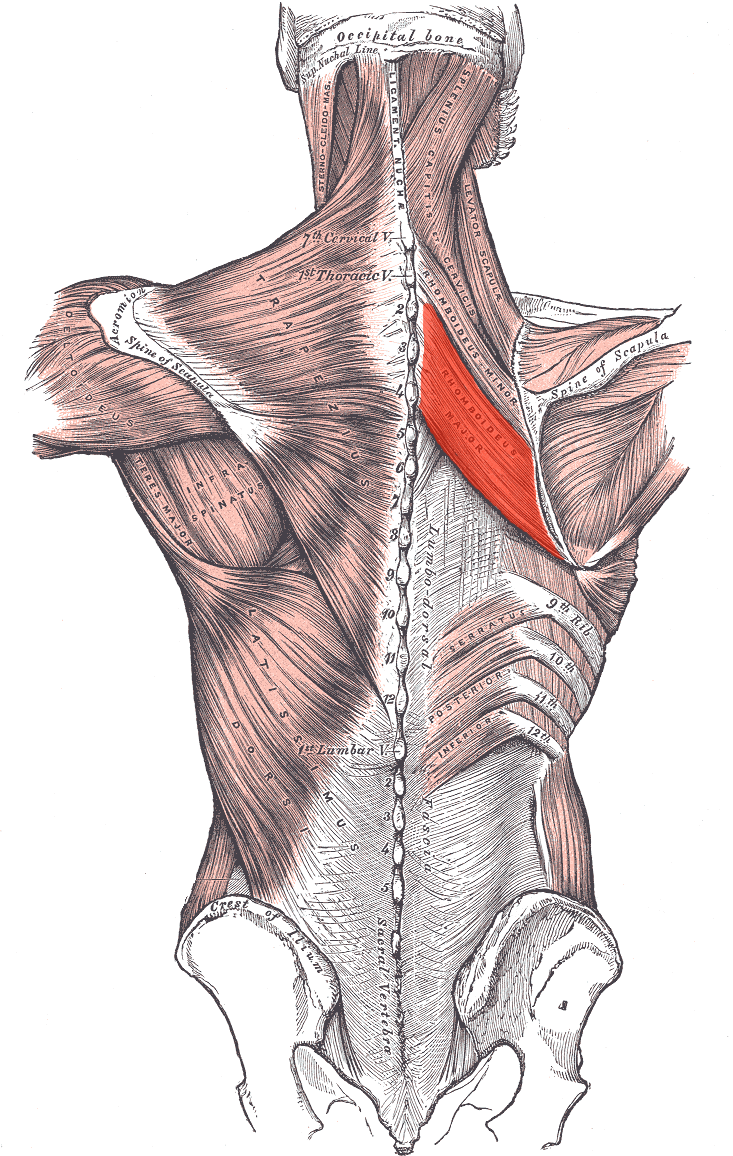
Identify the nerve that supplies the marked structure.
All are true about the thoracolumbar fascia, except:
A 26-year-old woman experiences severe back pain from an automobile accident. CT scan shows that the L5 vertebral foramen is completely obliterated by the collapsed L5 laminae and pedicles. In this injury, which of the following structures is crushed?
A 25-year-old soldier suffers a gunshot wound on the posterior lower back and is unable to move his legs. A neurologic examination and magnetic resonance imaging (MRI) scan reveal injury of the cauda equina. Which of the following is most likely damaged?
Practice by Chapter
Vertebral Column
Practice Questions
Spinal Cord and Meninges
Practice Questions
Back Muscles and Fasciae
Practice Questions
Vertebral Joints and Ligaments
Practice Questions
Vasculature of the Back
Practice Questions
Innervation of the Back
Practice Questions
Clinical Aspects of Back Disorders
Practice Questions
Applied Anatomy of the Back
Practice Questions
Surface Anatomy of the Back
Practice Questions
Development of the Vertebral Column
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app