
Back — MCQs

On this page
Where does the main part of vertebral venous plexus lie?
Epidural space lies between:
All are TRUE about intervertebral disc, EXCEPT:
Membrana tectoria is continuation of:
Which of the following parts of the vertebral canal shows the first secondary curve to develop?
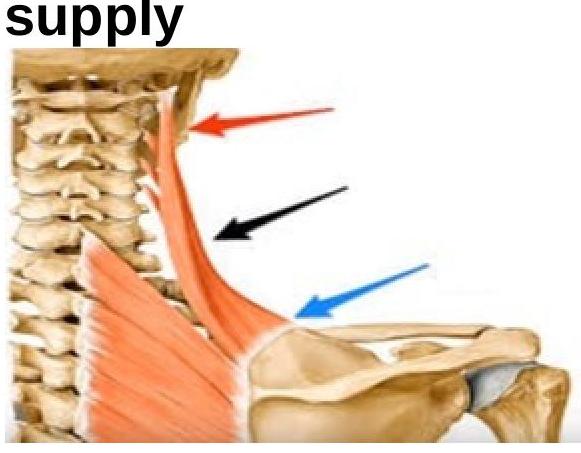
What is the nerve supply of the shown muscle?
All of the following contribute to the intervertebral disc EXCEPT:
In a lumbar puncture procedure, into which space is the needle inserted to access the cerebrospinal fluid?
Muscle lying between the anterior and middle layers of thoracolumbar fascia is?
Insertion of levator scapulae is?
Practice by Chapter
Vertebral Column
Practice Questions
Spinal Cord and Meninges
Practice Questions
Back Muscles and Fasciae
Practice Questions
Vertebral Joints and Ligaments
Practice Questions
Vasculature of the Back
Practice Questions
Innervation of the Back
Practice Questions
Clinical Aspects of Back Disorders
Practice Questions
Applied Anatomy of the Back
Practice Questions
Surface Anatomy of the Back
Practice Questions
Development of the Vertebral Column
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app