
Variations in Musculoskeletal System — MCQs

Tardy ulnar nerve palsy is most commonly associated with which of the following fractures of the humerus?
Which of the following clinical findings is characteristic of both osteomalacia and rickets?
All are true about osteoarthritis, except
Pronator teres syndrome is related to which nerve?
Which of the following structures does not pass through the greater sciatic foramen?
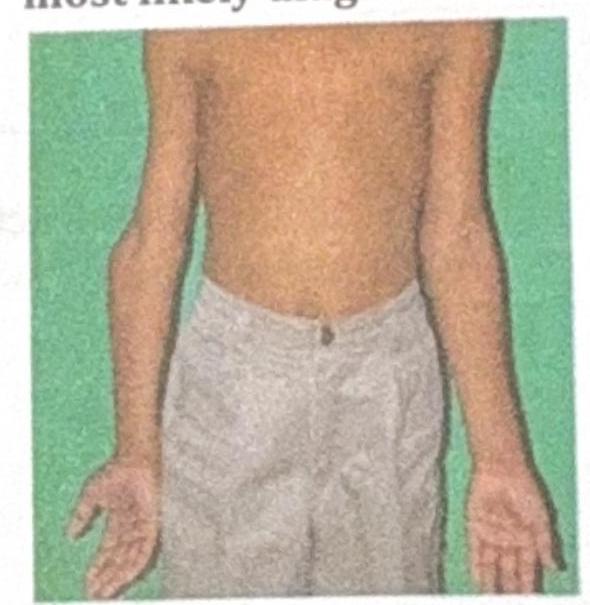
A 10-year-old boy presents with the physical findings shown in the image, characterized by inward angulation of the elbows. What is the most likely diagnosis?
Block vertebrae are seen in which condition?
Foot eversion is caused by
Statement 1 - A 59-year-old patient presents with flaccid bullae. Histopathology shows a suprabasal acantholytic split. Statement 2 - The row of tombstones appearance is diagnostic of Pemphigus vulgaris.
Which testis is typically positioned higher?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app