
Anatomical Variations and Anomalies — MCQs

On this page
A tooth characterized by a single conical cusp and a single root is classified as:
What differences can be seen in skulls of male and female before puberty?
Which is best used for sex differentiation?
Which of the following is an aberrant epiphysis?
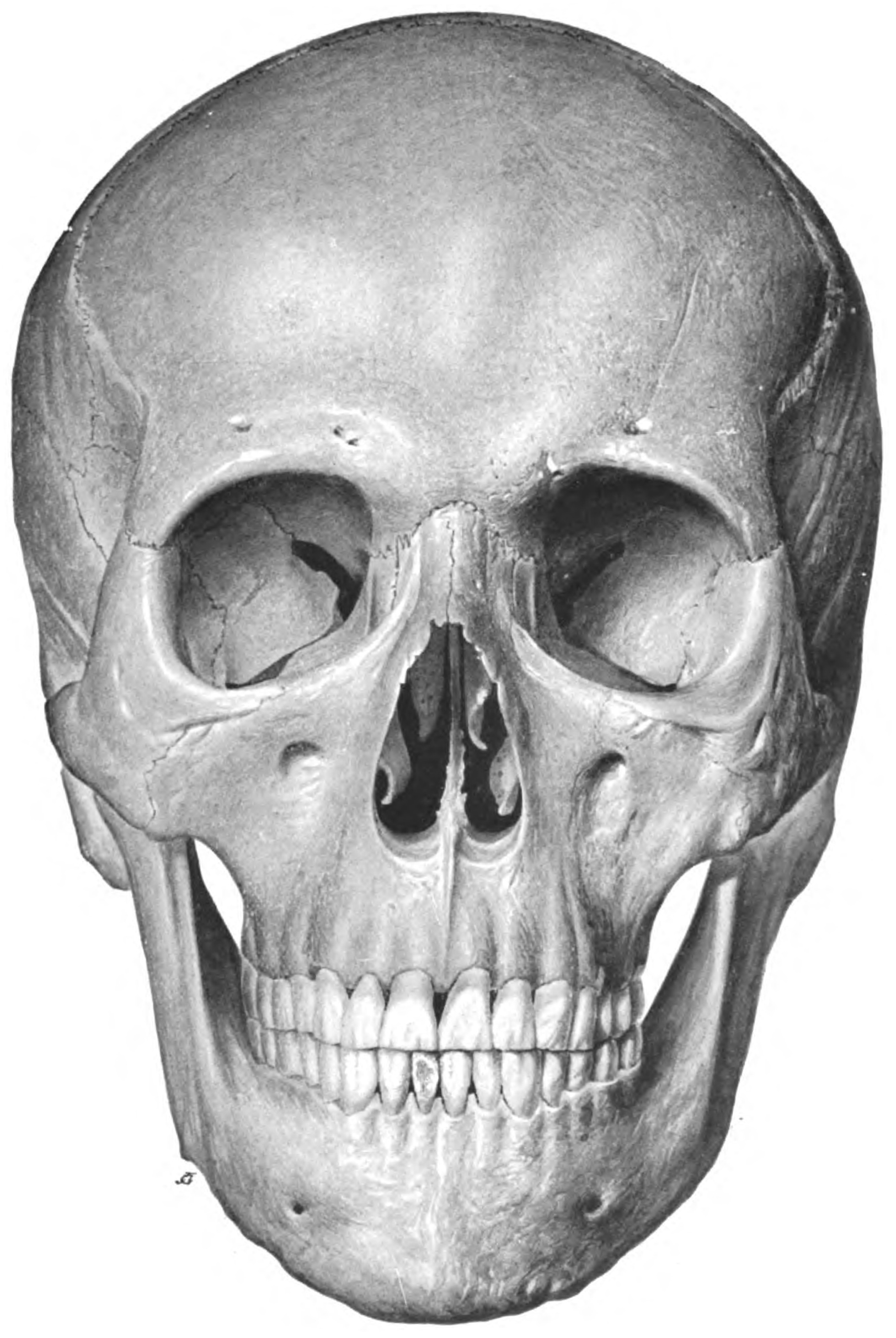
True statement about the skull shown below:
If both the alae of the sacrum are absent, it is called:
Which tendon is frequently absent in the upper limb?
A 45-year-old woman presents with severe headaches and is found to have a berry aneurysm. Which anatomical structure is most likely involved?
A surgeon notes increased bleeding during a splenectomy and suspects an anomaly in the vascular supply. Which variant of arterial supply could be responsible for this unexpected complication?
A patient presents with acute appendicitis. Upon reviewing the CT scan, the radiologist notes an abnormally positioned appendix. What anatomical variation could explain a hidden appendix that was not detected during a physical examination?
Practice by Chapter
Principles of Anatomical Variations
Practice Questions
Variations in Vascular Anatomy
Practice Questions
Variations in Musculoskeletal System
Practice Questions
Variations in Nervous System
Practice Questions
Variations in Visceral Anatomy
Practice Questions
Clinically Significant Anatomical Variations
Practice Questions
Congenital Malformations
Practice Questions
Genetic Basis of Anatomical Variations
Practice Questions
Surgical Implications of Variations
Practice Questions
Imaging Aspects of Anatomical Variations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app